







Classification of Vascular Lesions
The most unscientific terms of diagnoses by doctors are vascular lesions, such as port-wine stain (PWS) and strawberry hemangioma. These terms were made in the past when doctors in Western countries thought that these conditions were caused by eating strawberry, wine or salmon during pregnancy, but a lot of doctors are still using these terms today. Using food for naming diseases reflects how unscientific and ignorant people were in those days. There is a saying in China that calling the accurate name is the first step for understanding a thing. Hemangioma and vascular malformation are two different entities, as shown in their names, although skin hemangioma and vascular malformation are often called hemangioma together. Even pathological reports divide lesions of thin blood vessel as capillary hemangioma and those of thick blood vessel as spongiform or cavernous hemangioma, regardless of the presence of tumor or malformation. Hemangioma and vascular malformation have completely different pathogenesis, different component blood vessels and blood flow rate, and even different therapeutic effect and prognosis.

[Advertisement] COPPER BROMID(Yellow/Green Laser) – Manufacturer: BISON(www.bisonmedical.com)
International Society of Study of Vascular Anomaly (ISSVA) differentiates hemangioma and vascular malformation as follows:
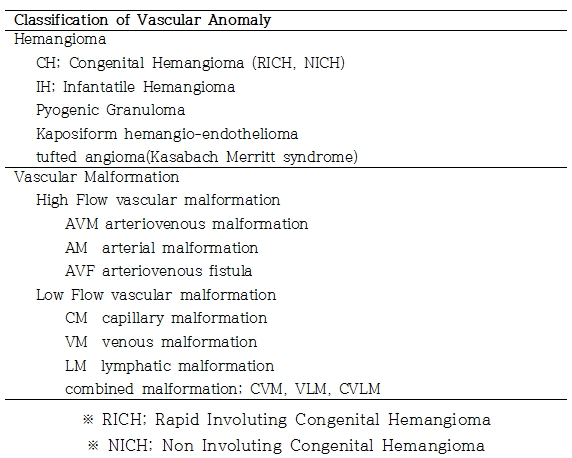
In terms of pathological difference, hemangioma, being a tumor on blood vessel, shows clear endothelial proliferation, compared to vascular malformation, which does not. What makes hemangioma different from vascular malformation is mast cell proliferation and thickening of basement membrane.
Progress and Prognosis of Vascular Lesions
Hemangioma is the most common tumor in infants. It may develop on the skin, as well as limbs, chest and abdomen; it may even be left unnoticed in some cases. Most cases are infantile hemangioma (IH), or congenital hemangioma (CH) in rare cases. The onset of CH starts from after birth. It appears elevated in the center and flat around the border, with white trim. CH can be divided to rapid involuting congenital hemangioma (RICH) and non-involuting congenital hemangioma (NICH). The latter is seldom treated by laser therapy and requires surgical treatment in most cases. IH, which is a commonly encountered hemangioma, is rarely observable after birth but grows rapidly by 1 year after birth, after which comes a stagnant period, followed by spontaneous regression. The spontaneous regression period comes at different age for each patient; approximately by 7 years old in 70% and by 9 years old in 90%.
Hemangioma undergoes proliferation phase (before 1 year old), involuting phase (1-7 years old) and regression phase (after 7 years old); however, vascular malformation does not have involution and tends to grow with age. Doctors often prefer to wait and see when they encounter a vascular lesion, because they cannot differentiate hemangioma from vascular malformation. Skin capillary malformation has higher cure rate when treated early with laser, but a number of patients visit past their optimal therapeutic period.

Figure 1. The involution of hemangioma could be advanced by local steroid injection and laser therapy every 1-2 month(s) for a rapidly growing hemangioma in a 4-month-old infant

Figure 2. Hemangioma leaves scar or abnormal skin in 50% after spontaneous regression, requiring plastic surgery
Vascular malformation has very different appearance depending on the component blood vessel; arterial malformations, such as arteriovenous malformation (AVM), arteriovenous aneurysm and aneurysm, and often grow rapidly due to high flow and high pressure. Vascular malformations with high flow is amenable to pulse diagnosis, and strong arterial sound can be heard easily by Doppler. Recent 3D angio-CT allows three-dimensional visualization of vascular malformation, which is very helpful for therapeutic decision making.
Vascular malformation of capillary, vein or lymph node has low flow and few abrupt change. Mixed vascular malformation is a combination of capillary, lymph node and venous lesions. Vascular malformation may develop in young age as well and does not regress but is rather aggravated with age. In venous malformation, calcified beads may appear with age in the venous, which can be visualized by simple radiography.
PWS, a common facial lesion, is accurately termed as facial superficial capillary malformation. The thinly distributed skin lesion is well treated by laser. Since the capillary becomes thicker with age, younger patients have higher cure rate. Capillary malformation in middle-aged patients is thicker, particially elevated, and even accompanies hemorrhage.
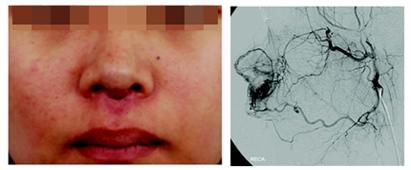
Figure 3. AVM of the nose, involving a number of arteries and veins, is gradually growing. Facial lesion, supplied from bilateral and cardiac circulation, requires extensive resection to prevent a recurrence, but such a decision is difficult to make, considering the patient’s appearance
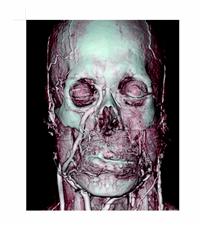
Figure 4. 3D angio-CT allows three-dimensional visualization of the distribution and appearance of vasclar malformation
Reference: Laser Plastic Surgery, Koonja Publishing, 2008, Seoul
- To be continued -
▶ Previous Artlcle : #5. Fractional Laser
▶ Next Artlcle : #7. Laser Treatment for Hemangioma and Vascular Malformation Ⅱ
























