







‘Best Lecture’ introduces famous lectures in dermatology and plastic surgery held in Korea. This will provide you with the opportunity to see distinguished lectures regardless of time and place. The lecturer of this lecture is Dr. Kim Il-hwan, Professor of Dermatology in Korea University Ansan Hospital. This is the summary of his recent lecture at ‘Lasers and Optical Medical Devices Study Group’. <Editor’s note>
Let’s look at the development of laser technology in dermatology first. The course of laser technology development was made in attempts to solve various dermatological conundrums as below:
Facial rejuvenation lasers have been also developed for the following skin changes from photoaging.

What makes laser technology applicable to such a variety of diseases is in the nature of laser. Monochromaticity (single pulse, an important factor for treating a specific disease) and selectivity to chromophore (coherence) of laser allow selective damaging of a target with highly absorbable, bright energy. This means that laser is capable of treating a particular target (water, Hgb, pigment or fat) of a certain disease with minimum damage to normal tissues. Therapeutic theories and technologies based in these properties of laser will be discussed in the following order:
First, Nonselective Surgical Laser Technology is applied to CO2 laser.
The mechanism of action of CO2 laser is nonselective, photothermal effect. It is capable of incision, excision, vaporization, debulking, coagulation, hemostasis and athermal photoactivation for treatment. Because of its nonspecific activity on the epidermis, it needs a technology to minimize thermal injury to the surrounding tissues of each lesion. This may need time and experience, and an understanding that the skill level may determine the therapeutic outcome or occurrence of side effects.
CO₂ Laser Surgery: Epidermal Lesions
The second is the development process of Skin Rejuvenation Technology. For skin rejuvenation, chemical peels, particulate resurfacing or electrosurgical ablation was used before the advent of laser. All these procedures were not widely accepted due to the risks greater than benefits. The development of laser technology allowed resurfacing of only targeted layer, contributing to minimizing side effects compared to before. Below are the Laser Skin Rejuvenation Techniques:

The development of Skin Rejuvenation Technology was made by a compromise between patients’ needs to minimize the downtime, even at the cost of slightly less effect, and doctors’ needs to have a technology with an efficacy as great as possible and few side effects. As a result, currently available lasers, including Non-Ablative Fractional Laser, tend to have less effect by a single procedure and require multiple procedures.
[Advertisement] ULTRA THIN WALL NEEDLE – Manufacturer: AESPIO(www.aespio.com)
In a recent clinical and histological study comparing Ablative Fractional Laser and Non-Ablative Fractional Laser, Non-Ablative Fractional Laser produced histologically a Microscope Treatment Zone (MTZ) and ablation with Ablative Fractional Laser also produced a microscope ablative zone (MAZ). The two were clinically not different. After all, skip area facilitates rapid wound healing, thereby reducing erythema from continuous scar or pigmentation. Now it is recommended to limit treatments to within 15% of the face in white people. Among NAR technologies, ablative FXL is the most advance anti-aging therapy for patients not responding well to NAFXL. Ablative FXL can induce more favorable recovery process, while minimizing damages to the surrounding tissues, after the treatment. However, dermo-epidermal junction damage may aggravate the degree of early inflammatory response and burning sensation. It also need repeated treatments to yield a sufficient effect. A recent study comparing 4 types of AFXL for their effect on developed photo-aging skin reported efficacy for wrinkle and skin texture but not for pores, recurrence of lentiginosis, and no difference among the devices. Considering such a little effect on skin tightening compared to a full-face ablation technology, NAR technology is now applied mostly to scar treatments, including acne scar. No downtime and low risk, as well as partial collagen remodeling effect, made it a suitable therapy for scar treatment.
The third is the Selective Photothermolysis (SPTL, SP) for melanin pigment and OxyHgb. SP is considered the most important and fundamental concept for every medial laser therapy. Pulsed Dye Laser (PDL) is the most advanced technology for the treatment of vascular lesions. Recent studies have reported better outcome after adjusting the pulse duration, number of pass and other parameters. Because blood vessels of different depth and size have corresponding difference in energy level for coagulation, however, existing 585 and 595nm were not sufficient for treatment. A method to overcome this limitation was studied after 2006, which was to combine a short wavelength (595nm) with a long wavelength (1064nm).
A study found that PDL wavelength, well absorbed by oxyHgb, converts oxyHgb to metHgb, which absorbs Nd:YAG well. In this manner, deeper vascular lesions that were not responding to existing therapies could be well treated with a lower energy, with minimal risk of scar.
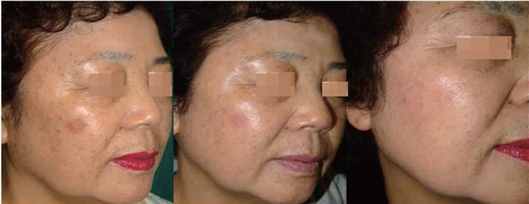
Now, let’s move on to the concept of laser toning, a pigment laser therapy that has recently gained a lot of popularity among Asians. This technology uses the concept of subcellular SP. For pigments in the dermis (including nevus of Ota and tattoo), the target area should be selectively damaged with a long wavelength delivered with high energy within a short period of time, while minimizing thermal injury to the surrounding tissues. On the other hand, inflammatory, dermal pigment disorders may often develop dyspigmentation from high energy; low energy is used to reduce such a risk, which is called a ‘laser toning.’
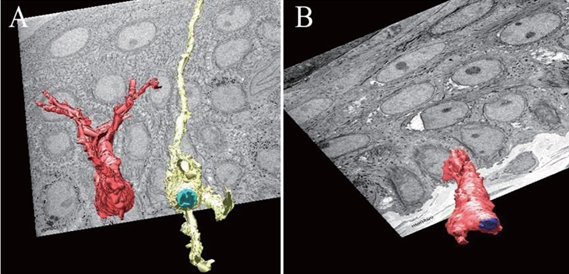
Decreased number of dendrite and 3D structures.(Ref. 5)
A. Before Laser Treatment. B. After 7th Laser Toning Treatment.
-To be continued-
▶ Previous Artlcle : #3-2. Current Laser Technology in Dermatological Field
























