







The ‘Best Lecture’ series introduces prominent lectures in dermatology and plastic surgery held in Korea. This series will provide you with the opportunity to enjoy distinguished lectures free from time or spatial constraint. The following lecture is given by Dr. Won Hyoung Kang, an authority in the treatment of pigmented lesions and director of Q Dermatology Clinic in Korea. Below is the summary of Dr. Kang’s lecture given at a seminar held by a laser manufacturer in Korea in July this year. <Editor’s note>

The target of melasma treatment with IPL or laser is melanin. Melanosome in melanocyte is about 0.5㎛ in diameter. The goal of IPL or laser is to apply adequate heat to the melanosomes.
Light is made up of photons, and travels 300,000km/s, which is not just a theory but a scientifically measured fact. Using this speed, we can calculate the accurate time it takes for laser or IPL to pass through a given melanosome, which is very fast of course; however, the speed of heat transfer (which is a critical issue) is approximately 1/100,000,000 of the speed of light within the human tissue. Absorbed photons transform into heat. Then certain time is required for the heat to get transmitted to the neighboring structures – here, we need to look at the concept of "pulse duration".

HELIOSⅡ/LOTUSⅡ/HYPERION – Manufacturer: LASEROPTEK(www.laseroptek.com)
This gives rise to the following question; what is the tissue heating time, 1 sec or 1 nsec? Heating for 1 nsec is not enough to deliver the heat to the neighboring structures. In other words, until the end of laser irradiation, the laser heat stays in the chromophores. It takes about 100-200 nsecs (0.1~0.2 μs) to heat melanocyte. Therefore, the success of laser therapy depends on the struggle against this time interval. The other question is whether to increase the temperature of the target structure highly or slightly, which involves the amount of "joules" applied.
Taken together, laser therapy involves setting the parameters of "pulse duration and joules" toward the direction you want.
Clinical Treatment of Melasma
It is common knowledge that melasma is very difficult to treat. In some cases, treatment worsens the condition, thus safety is an important concern in melasma treatment. It is critical to choose the safest treatment.
Clinically, melasma is not easily definable. A dermatologist will encounter patients with various types of melasma, and should be able to apply flexible techniques as needed for the treatment. Therefore, having a fixed formula for melasma treatment can be dangerous, as each melasma patient would benefit most from customized care.
This patient in <Figure 1> had pronounced marks on the cheekbone area like marks from wearing goggles. Other areas seem safe to apply IPL. This type seems to originate not from systemic factors, but a local pathology.
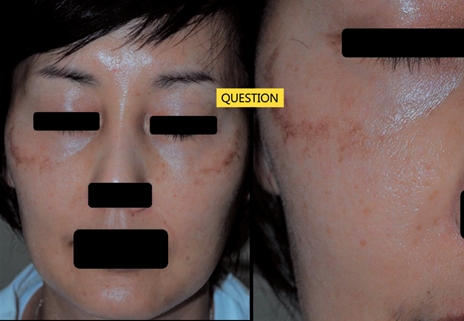
Figure 1
Type B in <Figure 2> illustrates a patient whose general skin tone darkens after IPL or laser therapy. The same approaches that are good for type A might be "dangerous" for type B – (as this type is likely to be aggravated by any kind of physical measures). This may be a systemic problem. Moreover, the lesions are not as pronounced as in Type A and this suggests that they arise from the dermis rather than epidermis. As the lesions arise from deep within, their presentation on the skin surface is less clear. Safety can be a problem in this type of patients. IPL with multi pulse and short pulse duration, as with E-Toning by Union Medical can be safely applied in this case. IPL can be more dangerous when the energy flows to the collateral structures particularly in this type of patients. Type C in <Figure 3> shows melasma only on the upper side of the cheekbone. Other areas appear to be without problems. There is no known explanation for such localization. Melasma has widely varying presentations among patients and the reason for such diverse etiology has not been elucidated yet. Melasma treatment in this patient can be tricky.

Figure 2

Figure 3
<Figure 4> shows a 40-year-old patient, with melasma shaped like goggle marks. What is worth noting is that the patient received a skin graft for spot-removal (a coin-sized nevus) from a plastic surgeon 20 years ago. The skin behind the ear was harvested and transplanted. What is interesting is that the grafted area is spared from melasma development.
Considering the patient’s age, the area with lesion has been exposed to sunlight for 40 years, whereas, the transplanted area has been exposed for only 20 years. It is necessary to see if melasma also develops in this area 20 years from now.
This patient in <Figure 4> received a skin graft from a plastic surgeon for a burn scar removal. The patient complained of hyperpigmentation along the suture even one year after the operation. What is interesting is that the scar is depigmented and the surrounding tissues are hyperpigmented.
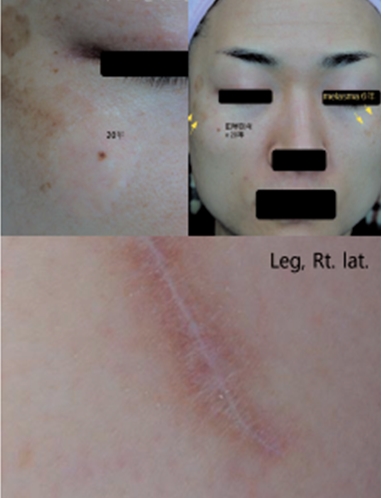
Figure 4
-To be continued-
▶ Previous Artlcle : #7-2. Melasma Treatment: Basic Principles & Clinical Applications
























