







Editor’s note: Dermatologic surgery was traditionally an area of dermatology. However, invasive procedures in dermatology have been losing ground to non-invasive procedures as patients prefer treatment with little downtime and no bleeding or anesthesia. Many experts still argue that dermatologists are better suited to perform surgery as they have expertise in normal and diseased skin tissues. In this light, D&PS starts a series of articles on the topic of dermatologic surgery. The author of this series is Dr. Jaehoon Park, Medical Director of Jeonju Beauty Clinic at Jeonju, Korea. Dr. Park is a dermatologist who performs various surgeries. We ask for our readers’ kind interest in the series.

The biggest obstacle for dermatologists to aesthetic dermatologic surgery would be lack of accurate anatomical understanding. This may be due to the fact that previous literature on anatomy focuses more on listing classical procedures rather than resolving practical challenges. Without appropriate anatomical knowledge, risk of failure and postoperative complications increase drastically.
I intend to share my experience in various surgeries with the readers in this new series on dermatologic surgery. It will provide in-depth yet straightforward discussions on anatomical challenges I have come across in my clinical practice. I will first focus on the anatomical terms of the skin surface, soft tissue structure, facial nerves, and fascia structure before going into the local anatomy of the head and neck.
[Advertisement] Aileen plus(Long pulsed Nd:YAG Laser) – Manufacturer: FineMEC(www.finemec.net)
A. Anatomy of the skin surface
Prior to dermatologic surgery, gross examination along with palpation of inner structure are carried out to assess the location and depth, etc. of the target and surrounding structure. Here, the structures to keep in mind are (from posterior to anterior); external, occipital, protuberance, zygomatic arch, orbital rim, supraorbital foramen or notch, infraorbital foramen, mental foramen, masseter, parotid gland and parotid gland duct, mastoid process, as well as various areas of the mandible and sternocleidomastoid(SCM), etc.
For example, the zygomatic arch can be used to prevent the temporal branch damage of the facial nerve and the supraorbital foramen can be used to locate the same nerve through nerve block. Unlike in healthy patients, parotid gland duct or the buccal branch of the facial nerve may be damaged in an elderly patient with hollow cheeks. Besides these anatomical structures, familiarity with detailed terminology of the skin surface structures is crucial for precision in surgery site marking and surgical technique.
These terms include; the eye (canthus, lacrimal punctum), nose (root, dorsum, tip, columella, lateral, sidewall, ala, nares, alar crease), cheek (nasolabial meloabial crease, modiolus), lips (vermilion border, vermilion zone, cupid bow, philtrum), and ear (auricle, ext, auditory canal, lobule, helix, antihelix, tragus, concha, fossa).
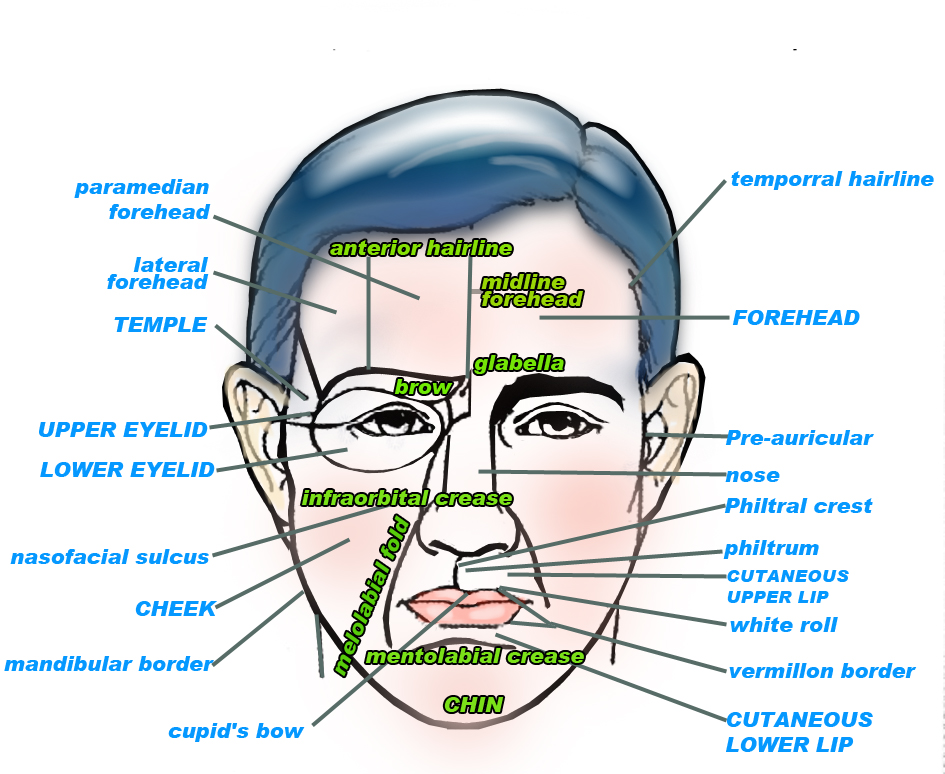
Figure 1. Facial cosmetic units (capital letters), forehead subunits (brackets), and junction lines.
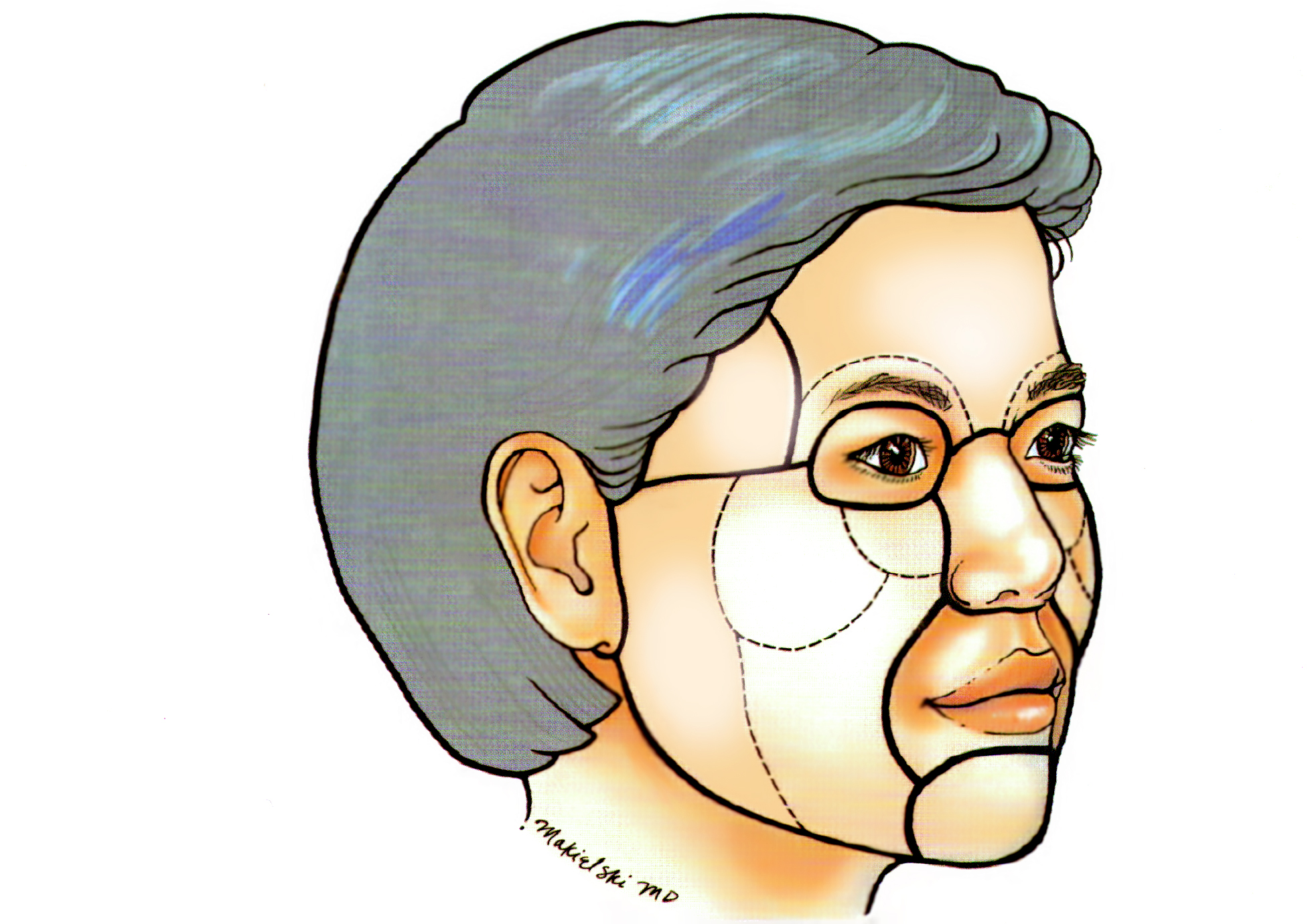
Figure 2. Facial cosmetic units.
On the other hand, the neck is often referred to as the anterior triangle between the SCM and central line and posterior triangle consisting of SCM and TRAPEZIUS. The face is divided into various parts based on the facial features. in 1954, Gonazaalez and Ulloa proposed the cosmetic unit or aesthetic unit (Figure 2) theory which explains the skin within a unit shows similar property in terms of the skin color, texture, hair, follicle size, sebum production and response to external stimulation, etc. According to this theory, excision or flap technique performed within this unit can bring the optimal aesthetic outcome.
This unit is divided by contour lines, for example, vermilion zone (line), eyebrow, eyelid margin, nasal contour and nasolabial fold, etc. This division differs depending on the scholar, however, they are categorized as following (shown in Figure); forehead [central, lateral (temporal), glabellar subunit], nose (dorsal, side wall, tip, alar, columellar), eye (upper & lower eyelid, medial & lateral canthal), lip (cutaneous upper & lower tip, vermilion zone), cheek [medial (subdivided into supermedial and nasolabial), lateral cheek (massertic), zygomatic, buccal)] and chin (chin proper, infralabil).
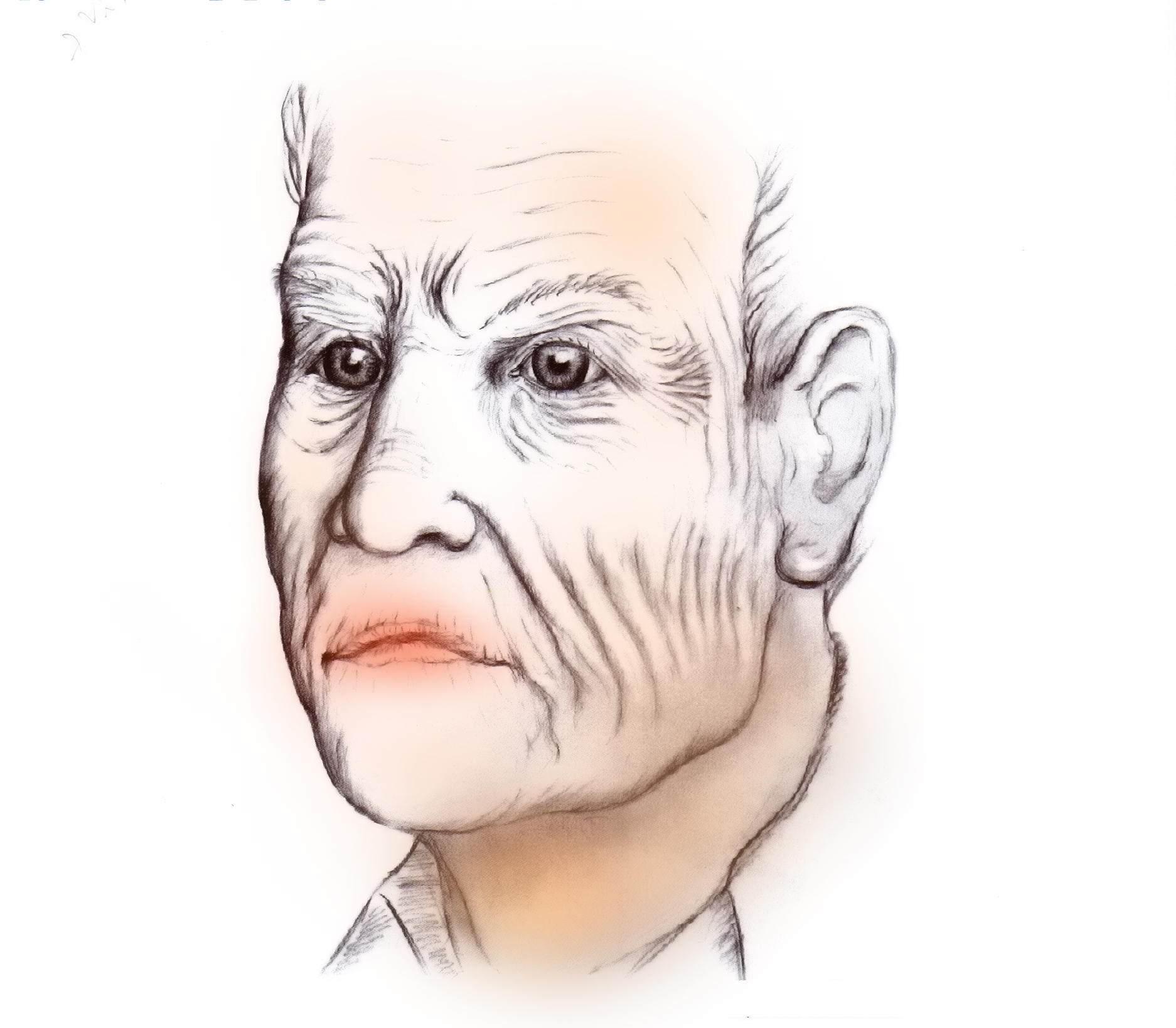
Figure 3. Relaxed skin tension lines.
As shown in Figure 3, the skin shows map-like lines under tension. These lines are called relaxed skin tension lines (RSTL, facial expression lines) which were defined by Borges in 1973. These lines are perpendicular to facial expression muscles and are caused by continuous contraction and expansion of the subcutaneous muscles. Other contributing factors include aging, gravity and chronic exposure to sunlight. In general, the facial wrinkles signify skin tension lines at a relaxed state. Incisions parallel to RSTL generally ease the healing process and bring good outcome. The temple and glabella creases conflict with the RSTL due to strong action of the local muscles.
The skin extends more easily perpendicular to RSTL (three fold) and the reciprocal tension is lower (0.5 fold) enabling easy suture and excellent postoperative aesthetic outcome. Unlike the wrinkle-prone facial skin, these lines are difficult to define in the body trunk and limbs. Examining the direction of the most noticeable creases or vellus hair may help.
-To be continued-
▶ Next Artlcle : #1-2. Anatomic Study of Skin Surface I
























