







▶ Previous Artlcle : #2-3. Anatomic Study of Skin Surface II
Eyelid fat consists of preseptal fat and postseptal fat. Presptal fat in the upper eyelid is also called retro-orbicular oculi fat (ROOF). It contributes to aesthetic curve and stretches toward preseptal components that contributes the curves of the eyebrow and supratarsal creases. Its counterpart in the lower eyelid is sub-orbicularis oculi fat (SOOF) which thins and generally does not cross the orbital rim. Postseptal fat is traditionally divided into two areas; two parts (lower and middle fat layers) in the upper eyelid and three parts (inner, middle and outer fat layer) in the lowr eyelid. Aging changes in periorbital areas include sagging of the oribiculairs oculi and surrounding soft tissues. The periorbital area eventually widens and orbital rim is pronounced.
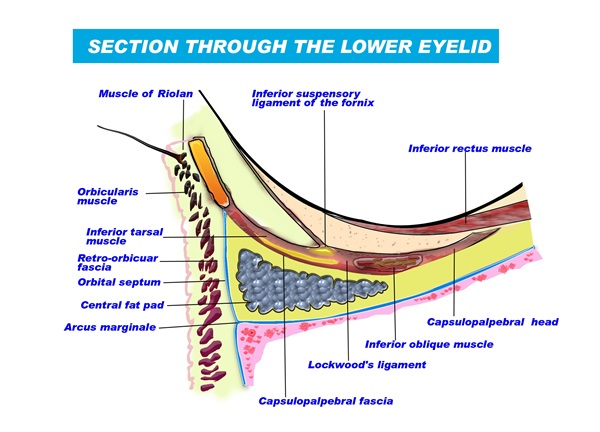
Also, fat protrudes through the weakened orbital septum in some cases. Lower eyelid orbital septum develops from thickened periosteum of the inf. orbital rim and it ascends surrounding the orbital fat to insert onto infratarsal margin. This orbital septum is divided by capsulopalpebral fascia into two similar parts. The upper part inserts into the tarsal plate lower margin as the capsulopalpebral fascia hugs the orbital septum again and protects the orbital fat from outward protrusion.

[Advertisement] Ultra Skin/Pastelle – Manufacturer: WONTECH(www.wtlaser.com)
However, the lower part not strengthen by the capsulopalpebral fascia is easily protruded due to an intraorbital pressure rise, excessive orbital fat, etc. creating a two layer appearance. Orbital fat may congenitally protrude through orbital septum, but in most cases the fat between the eyeball and infraorbital floor protrudes under orbital septum as aging loosens Lockwood ligament due to increased pressure. A palpebral bag develops from weakened orbital septum, obicularis oculi atrophy and lower eyelid sagging.
Tear trough groove forms due to relaxation of the tight attachment of obicularis oculi and orbital septum along the arcus marginalis and retro-inferior shift of the isthmus. The former can be corrected through orbital septum, orbital fat and sagging skin treatment but the latter is not resolved with such adjustments. Especially, cases of severe medial orbital fat protrusion with soft tissue atrophy and infraorbital rim skeletonization often fail to achieve satisfiactory outcome.
To correct the tear trough groove orbital septum can be pulled and fixed onto the infraorbital rim or orbital fat layer can be repositioned under or above the periosteum of the infraorbital rim (Figure4).
























