







The temporal hollowing that occurs with aging or excessive dieting is an indication for injectable filler or autologous fat graft. Temporal hypertrophy may be corrected by botulinum neurotoxin injection. The interest in the aesthetics of the temple area is increasing with the rising frequency of anchored-type thread lifting. Serious complications such as necrosis or vision loss are less common in this area, however, the risk of bleeding or neural damage still exists. As the tread is commonly fixed onto the temple area during anchored-type thread lift, accurate anatomical knowledge is necessary.

[Advertisement] MAGNUM(Q-switched Nd:YAG Laser) – Manufacturer: (www.i-dana.com)]
Terminology
The temple is one of the most anatomically complicated areas of the face. In this area, blood vessels, nerves, muscles and fat exist in many layers and scholars have not agreed on the nomenclature of different structures, frequently leading to confusion. The temporal region refers to the concave area inferior to the superior temporal line where the temporalis muscle originates from. Mendelson divides the face into five layers and as shown in <Table 1>, various terms are used to refer to the same structure. Superficial Temporal Fascia(STF) is called galea apneurotica superomedial to the temple and its name changes to temporoparietal fascia or mesotemporalis after passing the superior temporal septum(STS, also known as the Zone of adhesion or Zone of fixation). The fourth layer, loose areolar tissue, is also called subgaleal fascia at the temple and is divided into upper temporal compartment(UTC) cephalically, and Lower Temporal Compartment(LTC) caudally, based on the inferior temporal septum(ITS, also known as the orbicularis temporal ligament). The fifth layer, the periosteum, passes through STS and is divided into deep temporal fascia(DTF) inferiorly and periosteum that actually attaches to the bone. The DTF is also known as the temporalis fascia or temporal apneurosis, etc. In this article, I will use numbers and initials such as 1–Skin, 2-SubQ, 3-STF, 4-UTC & LTC, or 5-DTF to avoid confusion(Table 1, Figure 1).
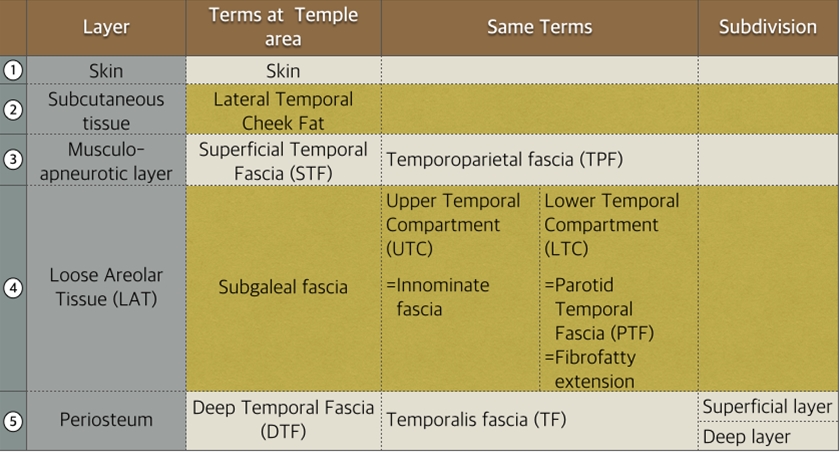
Table 1. Nomenclature of the temple region.
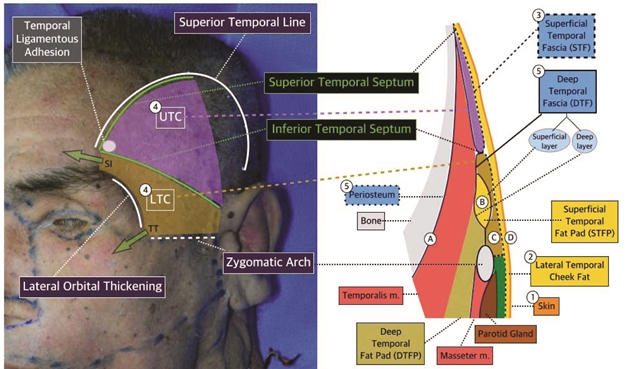
Figure 1. Anatomy of temple(TT: Temporal Tunnel, SI: Superior interval).
-To be continued-
























