







Many patients seek to improve their nasolabial folds with dermal filler injections. This is an area that novice doctors may feel rather confident about, however, even seasoned doctors find it challenging. The nasolabial folds are one of the areas with the highest risk of vision complications along with the glabella and nose.
Filler injection may suffice in nasolabial folds that are not too deep but thread lift is used in deeper folds. Very deep nasolabial grooves cannot easily be corrected with filler or thread lift and face lift could be considered. Experience and surgical techniques are necessary for correcting nasolabial folds but the doctor should also be able to select the most appropriate procedure for each patient. Knowledge about the aging process of the mid face is essential for establishing a treatment plan. One should also be well-versed with age-related changes in the retaining ligament and fat compartment as well as muscle movement and course of blood vessels, etc.
[Advertisement] ULTRA THIN WALL NEEDLE – Manufacturer: AESPIO(www.aespio.com)
Etiology
1. Gravitational theory vs. Volumetric theory
Most would say that nasolabial folds form due to sagging skin. While partially correct, this is not an accurate answer. If the lines are formed by upper fat pads (mainly malar fat) drooping due to the pull of gravity, lifting procedures should be used rather than dermal fillers. In the past, the main cause of mid face aging was the descent of malar fat but Rohrich and Pessa et al. revealed that the volume change of each fat compartment plays a more important role. With age, the superficial fat compartments grow in volume, whereas the deep fat compartments decrease in volume. Each fat compartment slightly bulge in the bottom and fall downward.
These changes are also seen in nasolabial folds. As shown in <Image 1>, the nasolabial fat, which is superficial fat compartment, descends as it grows in volume and the deep medial cheek fat (DMCF), which lies deeper than nasolabial fat, loses volume as it descends. The DMCF supports nasolabial folds and other upper soft tissues and when it weakens with age, nasolabial folds deepen. This is why the filler is injected in the deep layers in nasolabial fold correction. The DMCF lies medial to and beyond the boundaries of the nasolabial folds (Image 1). The filler injected in the DMCF lifts the nasolabial folds from underneath to straighten the folds.
Some say that Ristow’s space exists between the DMCF and maxilla and fat in this area is considered a separate deep fat compartment. However, such distinction is not significant in clinical practice and the fat in this area can be considered part of the DMCF.
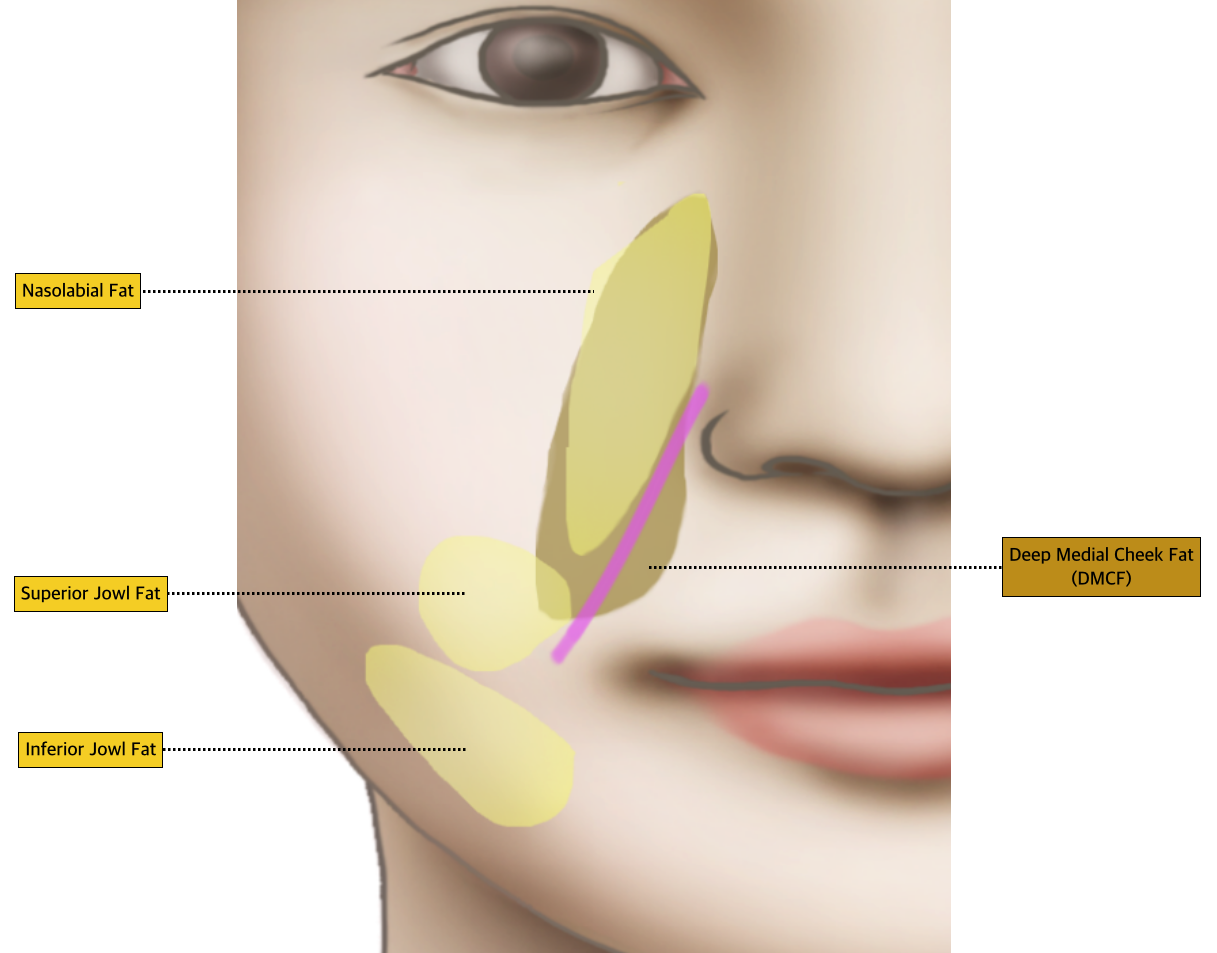
Image 1. Fat compartments- superficial vs deep.
-To be continued-
























