







2. Fascial theory vs. Muscular theory
We have discussed the age-related changes of the fat compartments. The question about what directly causes nasolabial folds still needs to be answered. What pinches the skin in this area to cause this deep fold? There are largely two theories that may be able to answer this question. First, fascial theory posits that the retaining ligament stretches all the way to the skin. There is slight controversy over the retaining ligament of this area but the maxillary ligament is generally thought to hold the skin in this area. The maxillary ligament is a true retaining ligament that connects the skin to the bone. According to the fascial theory, the maxillary ligament blocks the upper soft tissues from drooping further and this creates the fold.
The other explanation is the muscular theory. As shown in <Image 2>, this theory explains that the levator labii superioris alaeque nasi muscle, levator labii superioris muscle, and zygomaticus minor/major muscles directly connect to the skin and create the fold. I am not saying that these two theories are mutually exclusive but in my opinion, the muscular theory may provide a better explanation.

[Advertisement] FCR® (Fractional Prickle CoralCalcium Regentron) – Manufacturer: (www.illglobal.com)]
Here is why I support the muscular theory. Some say that the maxillary ligament is very strong. However, comparison of the tension of the true retaining ligament showed that the maxillary ligament was weaker than the zygomatic ligament, orbital retaining ligament (ORL), and mandibular ligament. Moreover, the location of the nasolabial folds do not coincide precisely with the attachment of the maxillary ligament to skin. On the other hand, the location of muscle attachment shown in <Image 2> coincides with nasolabial folds. Histologic findings also show that these muscle fibers connect to the skin, which adds more support to the muscular theory. It may not be clinically important which of the two theories is correct, however, theoretical knowledge is crucial in correcting imbalance in nasolabial folds or mouth corners using botulinum toxin injections.
Other anatomical factors that deepen the nasolabial folds may include depressed maxilla, thinner skin in the center of the fold, and variability of SMAS around the nasolabial folds, etc. With age, depression of the facial bone takes place in varying degrees and the maxilla is particularly indented around the nose. This, in turn, causes the DMCF depression and worsens the nasolabial folds. Moreover, the SMAS inside and outside the nasolabial folds have different histolotical characteristics. Simply put, the SMAS outside the fold is rich in fat, loose and thick, whereas, the inner fold SMAS is thinner with denser fat.
As discussed above, the nasolabial folds are caused by various factors and no single procedure can tackle all the etiological factors simultaneously. This is why some of the most experienced doctors find nasolabial fold correction challenging.
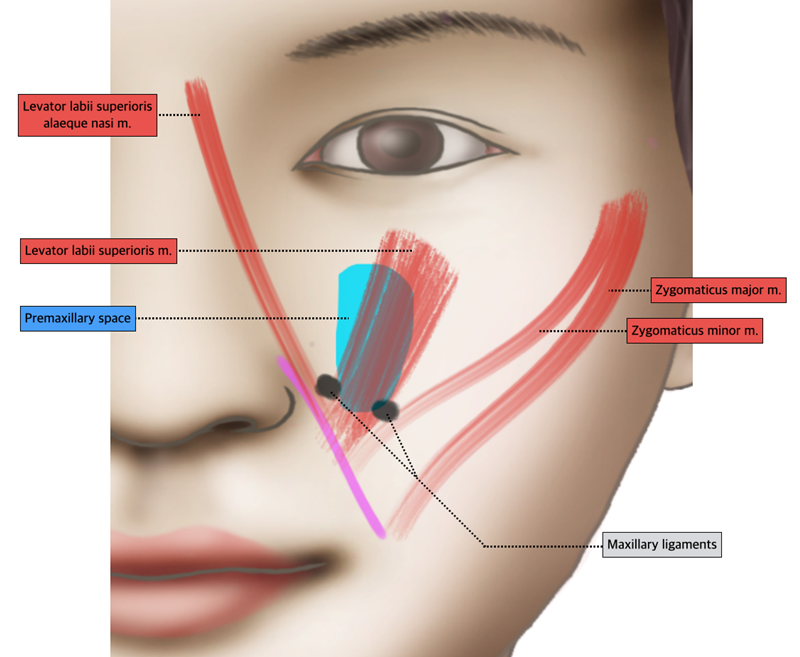
Image 2. Fascial theory vs Muscular theory.
-To be continued-
























