







Caution during treatment
The most important aspect of nasolabial fold correction using dermal filler is avoiding facial arteries. A lot of data on the course of facial arteries and vasculature related to nasolabial folds, etc. have become available. However, it is still very difficult to generalize due to wide variability between patients. One could come to the following conclusions based on the most convincing data. First, the facial arteries may lie in shallow areas about 1-2 cm laterally from the modiolar region (entering point). Second, blood vessels tend to rise upward from the lower part of the nasolabial folds toward the alar. Third, deep layers immediately above the DMCF or maxilla are relatively safe from the course of the facial arteries. Considering that the deeper layers are safer and the DMCF provides a lift for nasolabial folds, the layer immediately above the maxilla may be the optimal depth for dermal filler injection (Image 3).
I occasionally encounter patients who complain of superolateral migration of the filler despite inferomedial injection. Such migration may have been caused by insufficient blocking of the superolateral side during injection which could result in migration during treatment. Moreover, the movement of expression muscles may have shifted the filler to areas of lower resistance even if the patient did not massage or touch the treated area. The area that is particularly prone to filler migration due to low resistance is the premaxillary space marked blue in <Image 2>.
<Image 3> shows the fat compartments, muscles, space and course of facial arteries we have discussed so far. The green area marked with a star is the recommended filler injection area. I recommend using over a half of the entire injection amount in deeper layers. However, deep injections are not sufficient to correct excessively deep dents or folds. If the filler has to be injected into the superficial fat, practice particular caution as facial arteries could pass in that depth.
The nasolabial folds can also be corrected with thread lift. In such a case, the main target is the malar fat including the nasolabial fat and the thread should be inserted into this layer. However, thread lift without volume enhancement does not bring satisfactory outcome and combining a dermal filler should be considered.
We will take a look at tear troughs in the next article.

[Advertisement] A-One LITE(Facial Diagnosys System) – Manufacturer: BOMTECH(www.bomtech.net)
References
1. Gierloff M, Stohring C, Gassling V. Aging Changes of the Midfacial Fat Compartments: A Computed Tomographic Study. Plast. Reconstr. Surg. 129:263, 2012.
2. Wong CH, Mendelson B. Facial Soft-Tissue Spaces and Retaining Ligaments of the Midcheek: Defining the Premaxillary Space. Plast. Reconstr. Surg. 132:49, 2013.
3. Brandt MG, Hassa A, Roth K, et al. Biomechanical Pproperties of the Facial Retaining Ligaments. Arch Facial Plast Surg. 14(4):289, 2012.
4. Lee JG, Yang HM, Choi YJ, et al. Facial Arterial Depth and Relationship with the Facial Musculature Layer. Plast. Reconstr. Surg. 135:437, 2015.
5. Mendelson B, Wong CH. Changes in the Facial Skeleton With Aging: Implications and Clinical Applications in Facial Rejuvenation. Asst. Plast Surg. 36:753, 2012.
-To be continued-
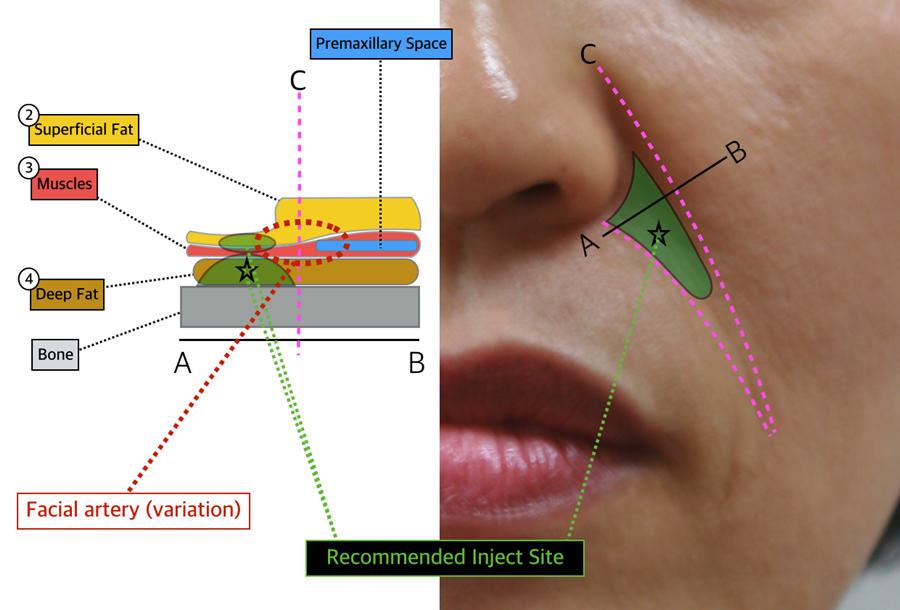
Image 3. Recommended inject site.
























