







Considerations for dermal filler correction of tear troughs
In the past, filler injection procedures of tear trough targeted the SOOF. After it was found that this layer lacks fat, the filler is injected into the orbicularis oculi muscle or subcutaneously. Shallow injections should use a soft filler due to lack of fat pads or sufficient post-injection massaging to avoid irregularities. The shape of tear troughs differ between upright and supine positions. Therefore, performing the correction in the supine position may cause unnatural looking to appear in the upright position. Any irregularities in this area of the face is particularly noticeable and cause patient dissatisfaction.
The three point technique was once used for injecting into deeper layers. No particular technique is currently favored for deeper injections. When injecting into the orbicularis oculi muscle, the filler should be placed as deeply as possible, otherwise, the orbicularis oculi muscle may contract and the filler can be accumulated.
The angular vein passes parallel and immediately under the tear trough and excessive movement of the needle or cannula can rupture the blood vessels and cause temporary bruising. The incidence of visual loss is much lower with tear trough correction compared to those reported with glabella, nose, nasolabial fold injections. However, caution is advised as the angular artery may ascend very close and medial to tear troughs. Pushing the medial canthal region with the doctor’s other hand during injection may decrease accident.
An accurate injection site is the most important aspect of treatment. The preseptal space is located superior to the tear trough and the premaxillary space is located inferiorly. It goes without saying that the filler should not be injected above tear troughs. As the tear trough ligament lies 4-6mm below the orbital rim, always palpate the orbital rim with the other hand prior to injection. If the filler is injected above the tear trough, it can increase the orbital fat herniation and worsen tear trough deformity (Image 1).
Tear trough correction is often combined with anteiormedial maxillary portion augmentation. However, the premaxillary space, DMCF, and SOOF lie under this region and deep injection may effectively provide volume to all these structures.
Lastly, one should practice caution to prevent the Tyndall effect. I recommended injecting the filler in deeper layers, but deep injection alone is insufficient to bring a good outcome. I sometimes inject a filler close to the surface to correct a noticeable superficial wrinkle. Here, one should be cautious about the Tyndall effect or translucence. Patient selection is important as the likelihood of Tyndall effect rises with thin and pale skin and shallow injection should be avoided in such skin type.
We will take a look at the Indian band in the next issue.
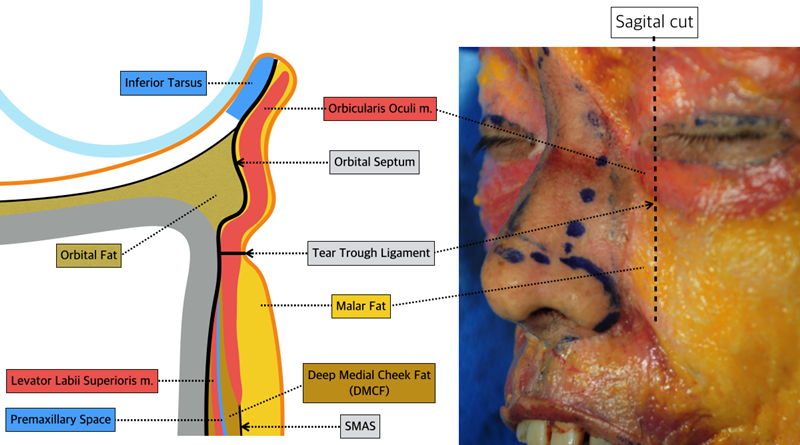
Image 1. Sagital view of the tear trough.
References
Huang YL, Chang SL, Ma L, et al. Clinical analysis and classification of the dark eye circle. International Journal of Dermatology, 53(2):164, 2014.
Stutman RL, Codner MA. Tear trough deformity: review of anatomy and treatment options. Aesthetic Surgery Journal, 32(4):426, 2012
Lambros V. Observations on periorbital and midface aging. Plast. Reconstr. Surg. 120:1367, 2007.
Wong CH, Hsieh MK, Mendelson B. The tear trough ligament: Anatomical basis for the tear trough deformity. Plast. Reconstr. Surg. 129:1392, 2012.
Haddock NT, Saadeh PB, Boutros S, et al. The tear trough and lid/cheek junction: Anatomy and implications for surgical correction. Plast. Reconstr. Surg. 123:11332, 2009.

[Advertisement] Tulip(Skin Tightening & Lifting) – Manufacturer: DANIL SMC(www.danilsmc.com)
-To be continued-
























