







Etiology of Indian bands
Various factors are involved in the creation of Indian bands.
First cause is the pull of the zygomatic cutaneous ligament, as mentioned above. This ligament has a strong pull over the descending upper structures and create a wrinkle.
Another cause could be the volume change of the malar fat. Malar fat is a thin fat layer and increases in volume and descends with age. Such drooping and thickening of malar fat makes the Indian bands more pronounced.
The third reason could be the reduced support by the orbicularis oculi muscle. The orbicularis oculi muscle and skin lose elasticity and tension with age. Due to such loss, tissues that were kept inside are now protruding outward.
The fourth and fifth reasons could be volume loss of the SOOF and caving of the maxilla. The SOOF is a thick fat layer and loses volume with age. Moreover, maxilla near the Indian bands cave toward the posterior vector with age. This caving of the bone acts to deepen Indian bands.
Lastly, the gliding effect of the prezygomatic space can contribute to creation of Indian bands. The prezygomatic space lacks ligaments that connect the base to surface and structures above it can easily descend.
Cautions regarding Indian band correction with dermal filler
The most important aspect of dermal filler procedure of Indian band is correctly identifying the patient conditions and determining the depth and amount of filler injection. As shown in <Image 3>, fillers can be injected into the deep and shallow layers. The primary target should be the skin insertion of the zygomatic cutaneous ligament where the wrinkle originates from. If the filler is injected above the origin and not the site of insertion, it enhances the upper tissues to thicken the malar mound and deepen the wrinkle.
In nasolabial line correction, volume enhancement is the key objective. Therefore, shallow layer injections are often unnecessary. However, Indian bands are primarily caused by the pull of the ligament on the skin and deep injections unaccompanied by shallow injection is not sufficient to correct the wrinkle. That is, deeper injections should be performed in patients desiring overall volume enhancement but shallow injections are recommended for correcting surface wrinkles.
Caution should be exercised during filler injection in this area to avoid the nerve and vascular structures. Particular caution should be given during deeper injections to avoid the infraorbital nerve that passes through the infraorbital foramen. This nerve passes immediately above the bone and originates from the lower eyelid, alar, lateral cheek and upper lip. Fortunately, the filler is rarely injected into the periosteum even when the injection is deep enough to reach close to the bone. Even very deep injections carried out with a needle and not a cannula tend to stay above the preperiosteal fat and the likelihood of damage is low.
Injections in the shallow or middle layers can reach the facial veins and facial arteries. Facial arteries sometimes pass immediately adjacent to the alar but often progress laterally in a detoured branch and caution is needed to avoid it. Rupturing the facial vein leads to severe post-treatment bruising and should be avoided. However, it is difficult to find the exact location of the vein without the use of specialized equipment. Slow and careful approach is needed during treatment.
We will discuss the anatomy of the nose in the next article.
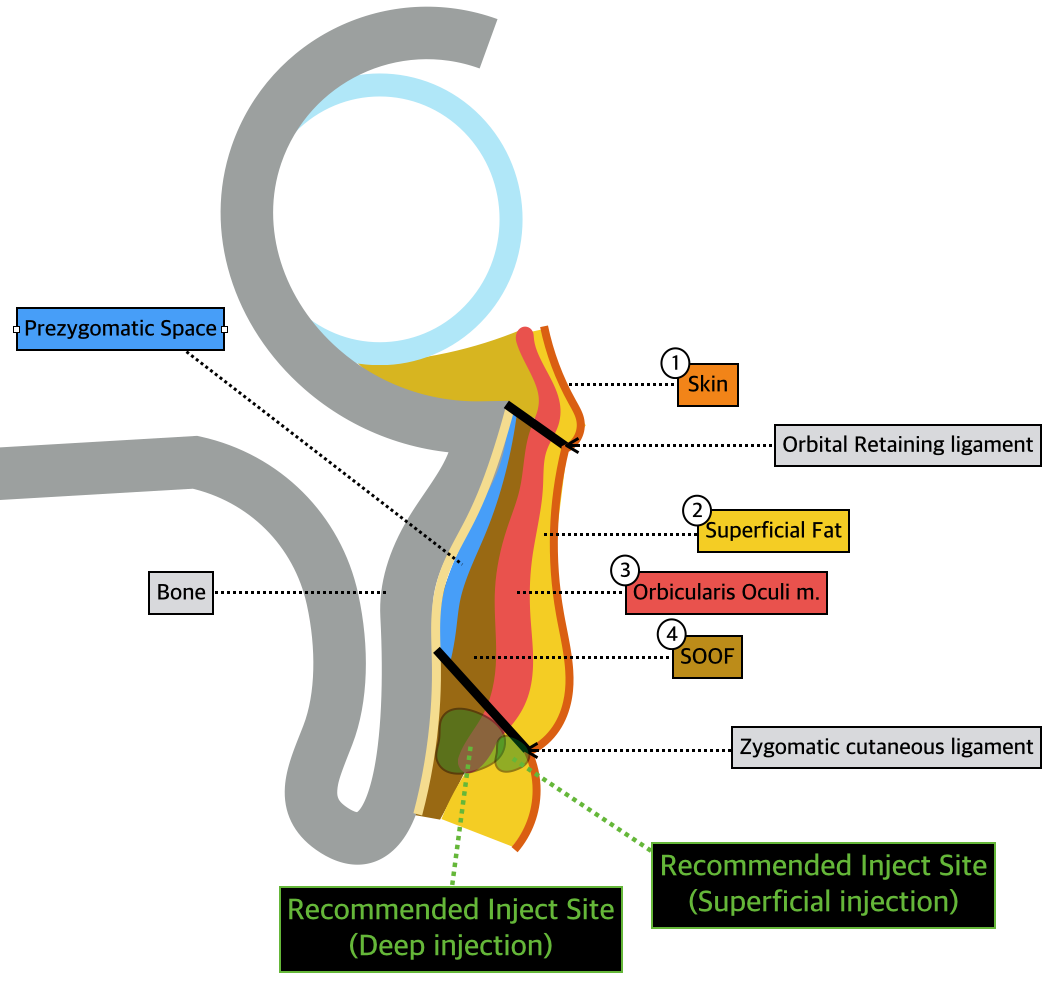
Image 3. Recommended inject site.

[Advertisement] MAGNUM(Q-switched Nd:YAG Laser) – Manufacturer: (www.i-dana.com)]
References
- Kpodzo DS, Nahai F, McCord CD, et al. Malar mounds and festoons: review of current management. Aesthetic Surgery Journal, 34(2):235, 2014.
- Mendelson BC, Jacobson ST. Surgical anatomy of the midcheek: facial layers, spaces, and the mid cheek segments. Colin Plastic Surg, 35:395, 2008
- Doubt G, Garb BB, Rampazzo A, et al. Surgical anatomy relevant to the transpalpebral subperiosteal elevation of the midface. Aesthetic Surgery Journal, 35(4):353, 2015.
- Mendelson BC, Muzaffar AR, Adams WP, et al. Surgical anatomy of the midcheek and malar mounds. Plast. Reconstr. Surg. 110:885, 2002.
-To be continued-
























