







Dr. Jung-whan Baek (H Plastic Surgery)
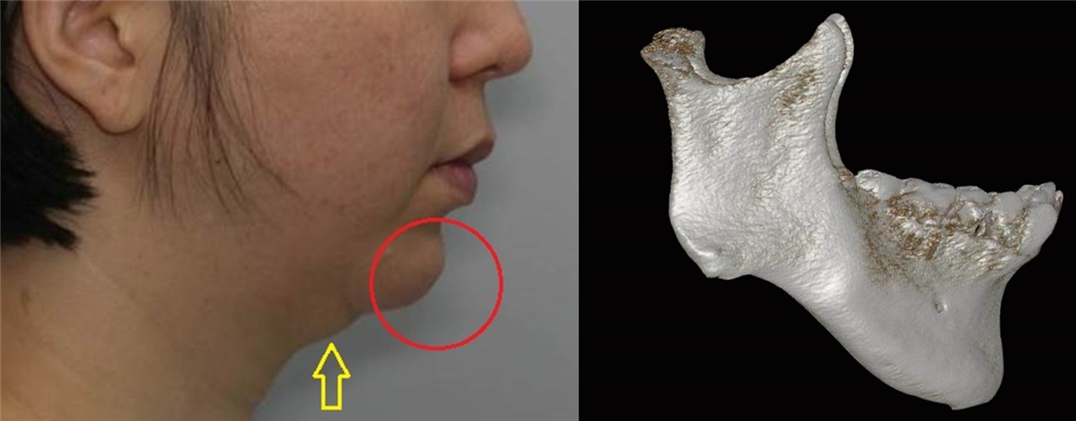
Image 5. A double chin can be seen from the side view, a common characteristic of patients with micrognathia and short chin. (Yellow arrow).
When mentum-cervicomental angle distance is short, soft tissues around the mandible remain and the geniohyoid muscle group that form the mouth floor shorten. This causes the skin and subcutaneous fat to lump together to create a double chin. The most ideal correction would be advancing the mentum along with the geniohyoid muscle group. SSRO or advance genioplasty can be carried out for chin advancement. Each method has its own disadvantages. In SSRO, the correction affects the maxilla and insufficient bone mass anterior to the gonial angle can create an undesirable shape of the mandible. Advance genioplasty alone cannot advance the chin beyond 6mm which is the limit for the plate to withstand the pull of the geniohyoid muscle group. Advance genioplasty is limited in micrognathia as the distance between the mentum and dental roots is also short.
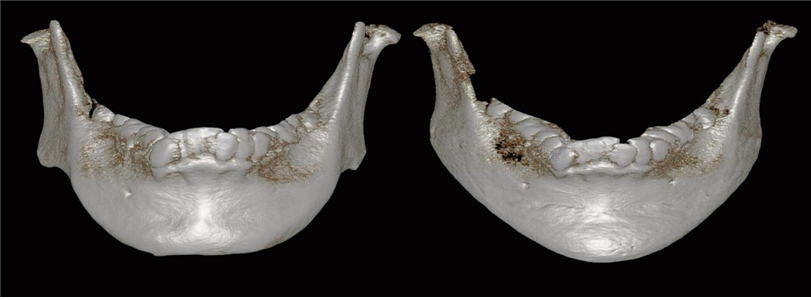
Image 6. 3D CT images before and after surgery. The vertical length of the chin has increased and the bone defect anterior to gonial angle has been corrected. Volume enhancement of the overall mandible has created the desired symmetrical shape of the mandible.
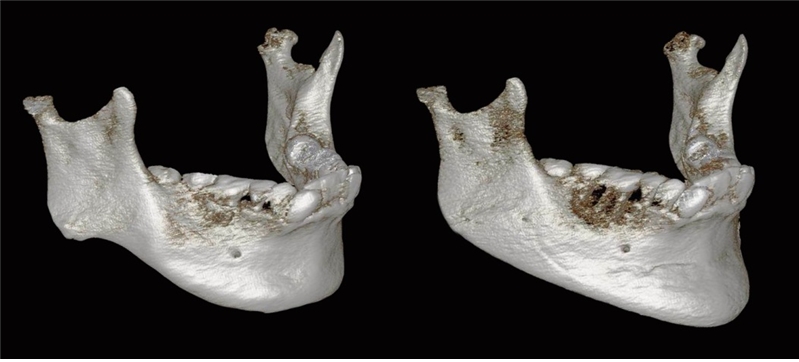
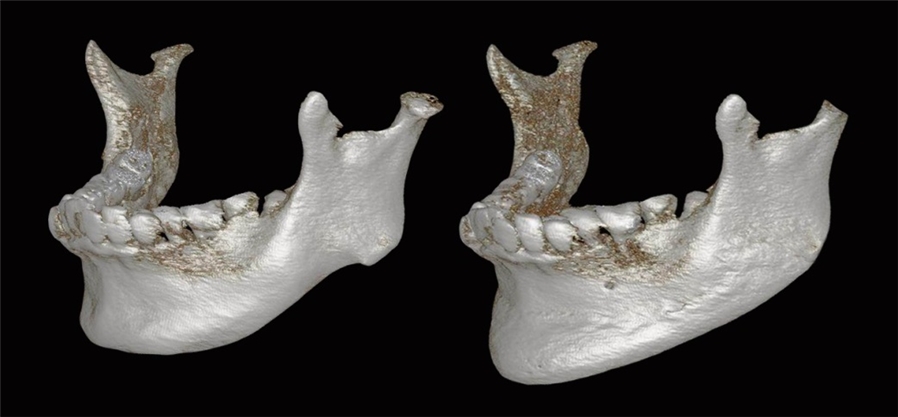
Image 7. Diagonal 3D CT images show that the implant has filled the bone defect anterior to bilateral gonial angle and enhanced the mandible body.
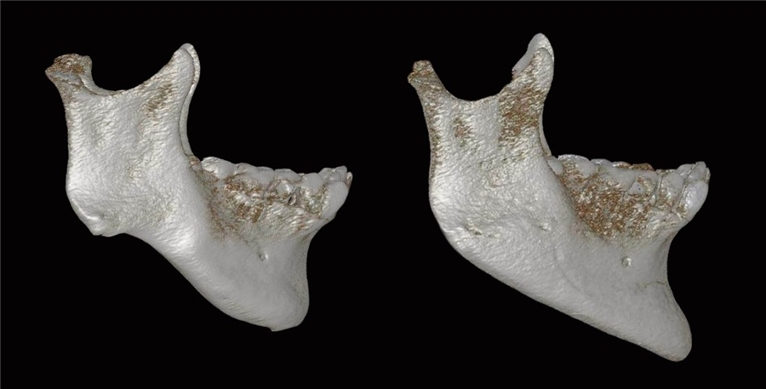
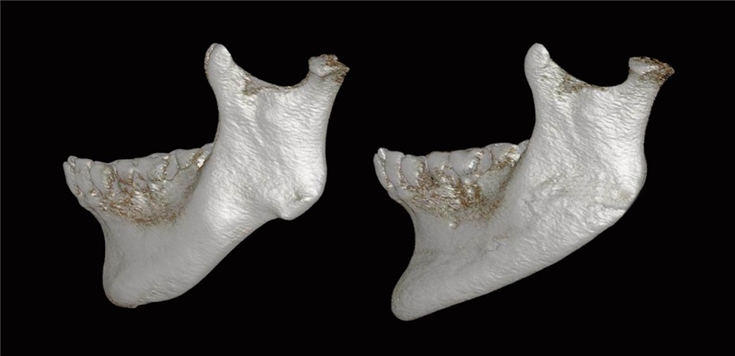
Image 8. 3D CT images from the right and left side view show volume enhancement of the mandible body and elongated mentum-gonial angle length.
When inserting the implant, preserve the mental insertion of the geniohyoid muscle group to correct the double chin. The double chin caused by lumped skin and subcutaneous tissues will expand and straighten due to the inserted implant.
-To be continued-
























