







Dr. Ahn Taejoo of Gyalumhan Plastic Surgery has served as an editor for Korean Society of Aesthetic Plastic Surgery and co-author of an American plastic surgery textbook. Dr. Ahn is currently on the review panel of Korean Society of Plastic and Reconstructive Surgeons. He gives frequent talks on his unique techniques of non-incisional ptosis correction. In this series, Dr. Ahn, who is particularly interested in obtaining natural outcomes, shares his knowhow on effective techniques for natural improvements in blepharoplasty, rhinoplasty and tightening procedures.
In this article and a few following ones, we will discuss latest techniques in blepharoplasty. First, we will take a look at double eyelid surgery, one of the most commonly performed procedures in Asians, as well as blepharoptosis(ptosis) correction, which is often carried out to improve the eye opening.
The double eyelid surgery can be defined as a procedure that creates an extra fold on the upper eyelid. That is, the fold forms when the eye is open. The eye area consists of various layers; skin layer, orbicularis oculi muscle(involving in closing the eyes), orbital septum, fat layer, levator palpebrae superioris muscle(involved in opening the eyes), Muller’s muscle, and conjunctiva. Looking at the lashes, the tarsal plate lies outside to conjunctiva, and Muller’s muscle attaches on top of the tarsal plate(Figure 1).
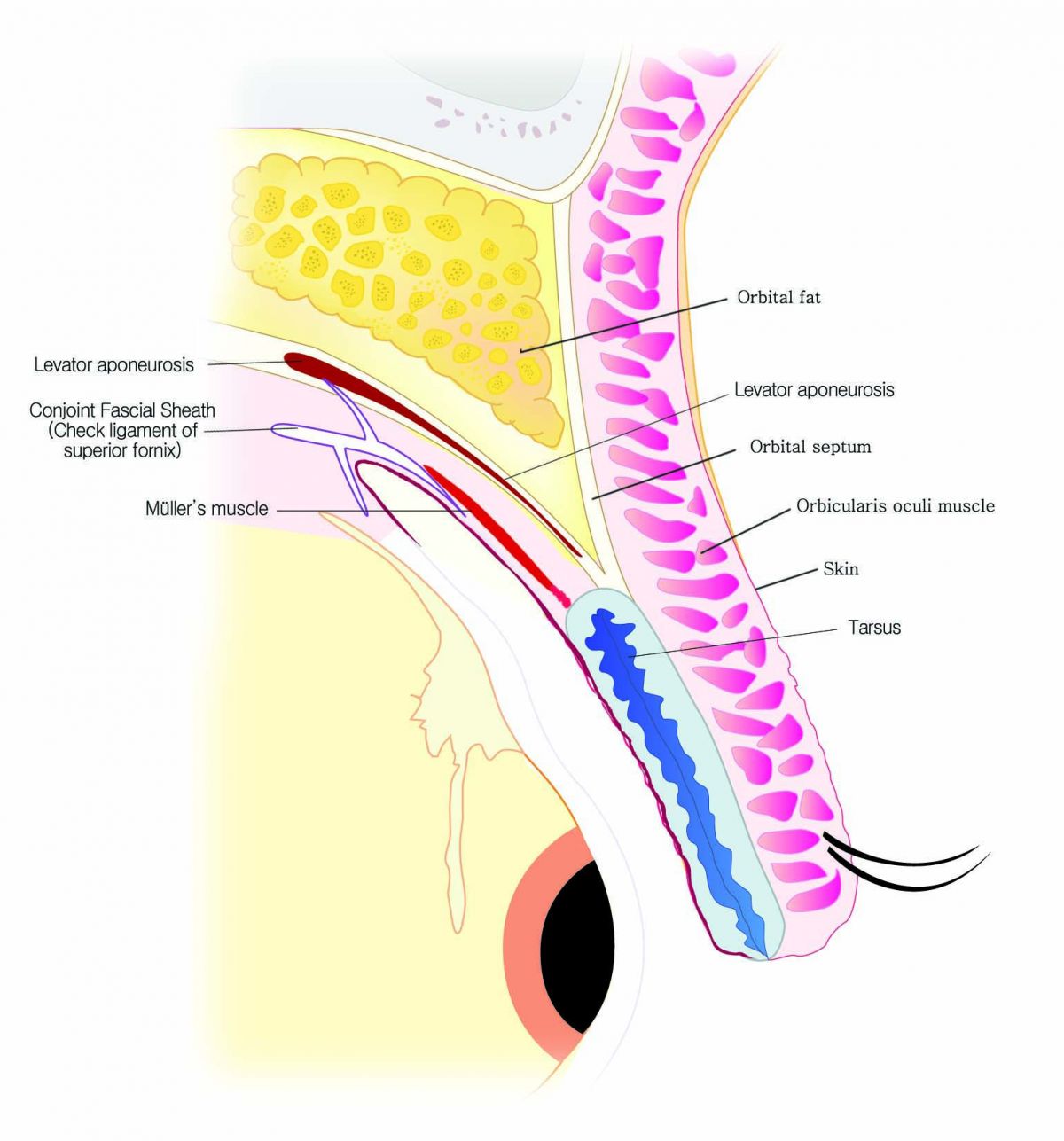
Figure 1. Anatomy of the eye area.
As the eyelid fold was generally placed on the tarsal plate in Asians, an incision was made to anchor the skin to the tarsal plate in the past. If the skin is attached to a fixed structure like the tarsal plate, the line appears during both closing and opening of the eyes, which was referred to as a static fold. This meant that a clear line was visible when the eyes are closed. Many Doctors are seeking to correct this nowadays. The recent trends favor creating a more natural static fold, by involving soft tissues. This allows fold creation similar to a dynamic fold that forms only when the eye is open(Figure 2).

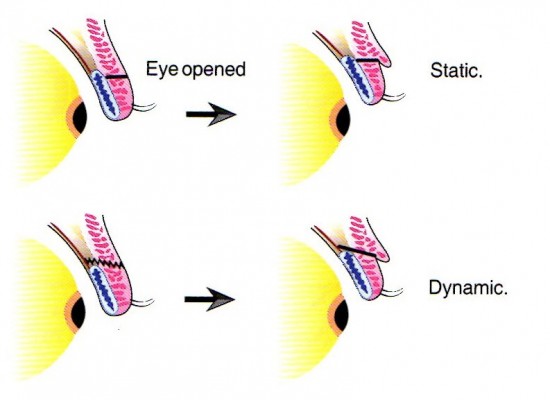
Figure 2. Diagram of a static fold and dynamic fold. The skin that is anchored directly to the tarsal plate is continuously pulled inward. If the soft tissues are also connected, they work as an elastic buffer, resulting in a weaker pull when the eye is closed, and a stronger pull when the eye is open. This can be compared to the difference of using an elastic string to pull back the Roman curtains as opposed to a non-elastic string.

[Advertisement] MAGNUM(Q-switched Nd:YAG Laser) – Manufacturer: (www.i-dana.com)]
Even with the dynamic fold, the resulting line may differ based on where the skin tissue is anchored. For example, if it is directly anchored to the levator aponeurosis, the resulting line is relatively strong and deep. On the other hand, if the skin is anchored to the orbital septum connected to the levator aponeurosis, the resulting line may appear more natural. However, as the pull is weaker, the fold may come undone later.
-To be continued
























