







▶ Previous Artlcle : #11-2. Treatment approaches for Basal Cell Carcinoma of Face in Koreans and Mohs Micrographic Surgery
Treatment
Different surgical methods are applied depending on the location and size of the BCC lesion. BCC occurring in areas with low recurrence such as the chest or limb can be effectively removed by curettage followed by electrocautery, cyrosurgery or traditional excision under local anesthesia, However, the likelihood of scarring and recurrence still remains. Deciding on an optimal treatment requires expertise as it differs depending on the size, infiltration depth, location, and histological form of the lesion. Mohs Micrographic Surgery (MMS) brings the best cure rate and aesthetic results in high-risk areas of the neck, center of the face and around the eyes (H-zone). MMS allows a phased incision of the lesion by examining a frozen section during the surgery and spares the maximum amount of healthy tissues.

[Advertisement] ATLAS(Long pulse 532nm & 940nm dual wavelength) – Manufacturer: MEDRO(www.medro.net)
The previous incision method removed at least 4mm of the normal tissue without microscopic examination of the 100% of the margins, therefore had a high risk of recurrence. The principles, concepts and stages of the MMS are as follows. Curettage is performed in the center of the lesion to allow microscopic examination of 100% of frozen section margins. The edges are beveled at a 45-degree angle. Preparation of the cross-section of the specimen for the frozen section examination and accurate mapping of cancerous cells with staining are particularly important processes of this procedure.
The stained specimen is placed under 400x microscope to check for remaining cancerous cells, a process which must be carried out by the operating surgeon. In a staged excision, only the area with remaining cancerous cells is removed with minimal excision of the healthy tissues. This way, complete removal of cancer cells as well as the best aesthetic outcome are possible. In Korea, this method has been introduced in university hospitals since the 2000s with limited application. MMS has been covered by national health insurance since a few years ago.
Indications and treatment effect of MMS in BCC
1. Indications(See Table 1.)
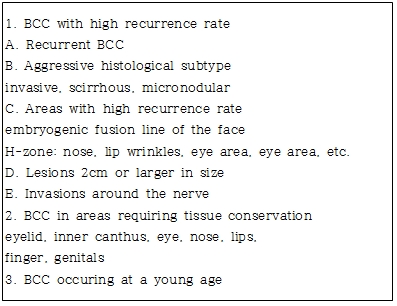
Table 1. Indications of MMS in BCC.
2. Treatment effect
MMS has the highest cure rate (5-year survival) among currently available skin cancer treatments.
(1) Recurrence rate of primary tumor by surgery
Mohs micrographic surgery: BCC 1.3% Surgical incision – 18%, Radiotherapy – 10%, Electrocautery -40%, Cyrosurgery – 12%
(2) Recurrent tumor
Mohs micrographic surgery: BCC- <10%
Tumor size:>2cm-15.2%, <2cm-7.4%,
Histological depth of the tumor: >4mm-17.2%,<4mm-
5.3% : Invasion of nerve tissue: BCC approximately 20%
Reference
1. JW Kim, CH Oh, IH Kim. Distribution of Histologic Subtypes of Basal Cell Carcinoma by Facial Aesthetic Unit and Subunit. Korean J Dermatol 2000;38(1):31~37.
2. KW Ro, SH Seo, SW Son, IH Kim. Subclinical Infiltrarion of Basal Cell Carcinoma in Asian Patients: Assessment after Mohs Micro graphic Surgery. Ann Dermat l ;23(3)276~281.
3. SB Son, SH Seo, SW Son, IH Kim. Original Article : Clinical Findings and Recurrence Rate of 123 Skin Cancers Treated with Mohs Microscopic Surgery. Korean J Dermatol 2008;46(1):8∼14.
4. Mohs FE: Chemosurgery, a microscopically controlled method of cancer excision, Arch Surg 42:279~295, 1941.
5. Mohs FE: The chemosurgical method for the microscopically controlled excision of cutaneous cancer. In Epstein E, editor: Skin Surgery, Philadelphia, 1956, Lea &Febiger.
6. Tromovitch TA, Stegman SJ: Microscopically controlled excision of skin tumors: chemosurgery(Mohs):fresh tissue technique, Arch Dermatol 110:231~232, 1974.
7. Gross KG, Steinman HK, Rapini RP. Mohs surgery. Fundamentals and Techniques. St. Louis, 1999, Mosby, Inc.
8. Snow SN, Mikhail GR. Mohs Micrographic Surgery, 2nded. 2005, Madison: The University of Wisconsin Press.
9. JH Park, JT Jeong, HJ Song, CW Oh, IH Kim. Case Report: Diagnostic Trial of Epiluminescence Microscopy in Two Cases of Pigmented Basal Cell Carcinomas(PBCCs). Korean J Dermatol 2001;39(10):1127~1132.
10. Altamura D, Menzies SW, Argenziano G, Zalaudek, Peter Soyer. Dermatoscopy of basal cell carcinoma:Morphologic variability of global and local featuresand accuracy of diagnosis. J Am AcadDermatol 2010;62:67~75.
-To be continued-
























