







CASE
▶ Patient: a 21-year-old woman
▶ Chief complaint: The patient visited the hospital for hard nodular lumps accompanying pain in bilateral earlobes growing bigger in size (duration: for 1 year).
▶ Past medical history and family history: She had received intralesional injection of triamcinolone for 1 year and pressure therapy for several months at a private clinic.
▶ Skin findings: Hard nodular lumps developed from ear piercing scars in bilateral earlobes (Figure 1).
▶ Diagnosis: Earlobe keloid solely based on clinical findings
▶ Treatment: Intramarginal excision (see Figure 5 below) immediately followed by radiation therapy (see the description below), resulting in full recovery without recurrence so far.

[Advertisement] DEPILIGHT(808 Diode laser for Hair Removal) – Manufacturer: DANIL SMC(www.danilsmc.com)
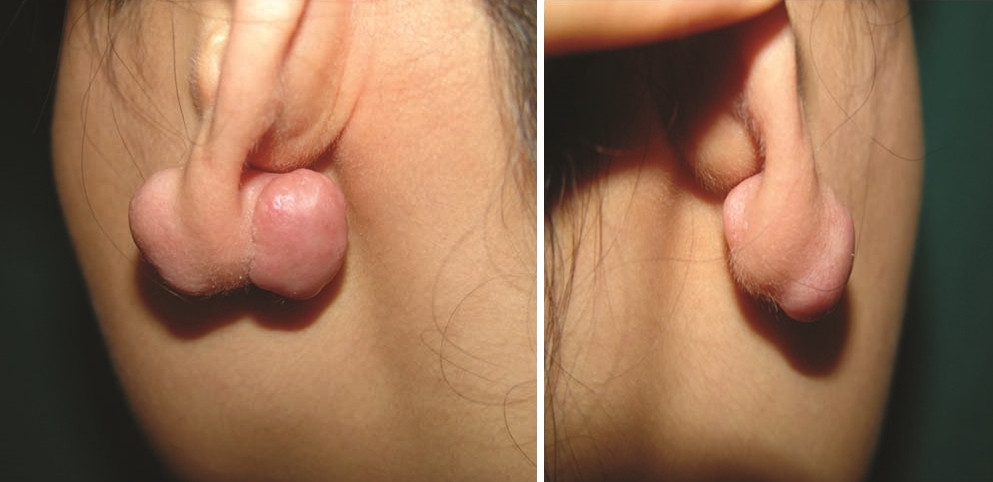
Figure 1. Hard nodular lumps in bilateral earlobes.
Histology findings: Postoperative histological images and histopathologic findings (see Figure 2).
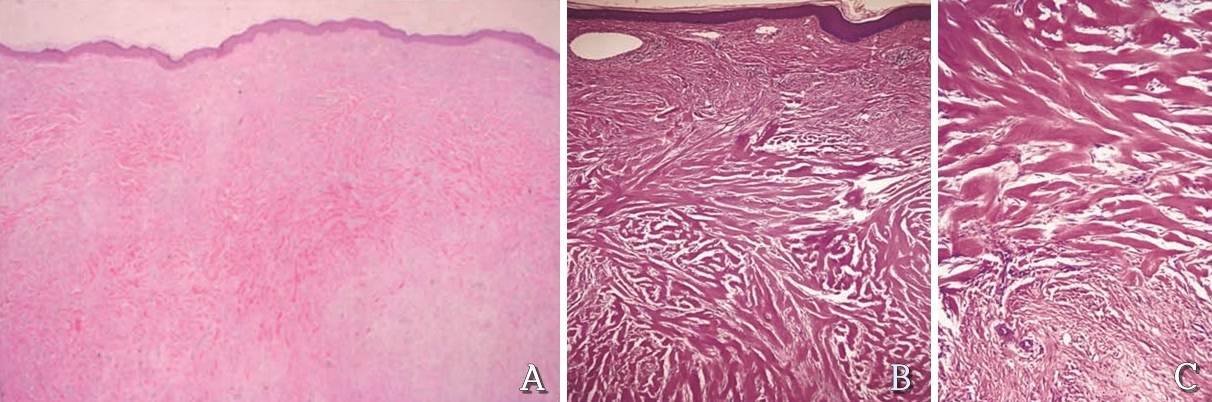
Figure 2. Histopathological findings of keloids (H & E, A, B, C)
Histopathologic findings of the keloids
1. Inside the scar tissue are thick hyaline collagen fibers, with homogeneous eosinophilic staining, proliferated disorderly and widely in bundle (A and B) compared to relatively normal collagens in the lower part (A and C).
2. Proliferation of skin fibroblasts and mucopolysaccharides, especially chondroitin-4-sulfate, is identified between collagen fibers.
3. The blood vessels are decreased unlike in hypertrophic scar or normal tissue recovered after injury.
Histopathologic findings of the keloids
1. Basic knowledge for earlobe surgery
• Skin in front of the ear: The skin is thin and directly attached to the cartilage without adipose layer.
• Local anesthetic injection induces a lot of pain. Tissue dissection and primary skin suture are difficult to perform.
• Skin behind the ear: Relatively thick and loosely attached to the lower cartilage.
• Cartilage: One cartilage shapes the ear. Cartilage injury should be monitored at all times because cartilage infection may develop to fulminant necrotic cartilage in rare cases.
• Auricular region: Wedge resection is available to approximately 1/4 of all, with tie-over dressing that passes through the cartilage.
• Occlusive treatment: Dressing should be removed within 3-4 days due to the risk of Pseudomonas aeruginosa infection, and complete occlusive treatment is contraindicated.
• When a large area of the soft tissue on top of the cartilage has been removed, making it hard to perform primary suture or to expect the formation of granulation tissue by secondary suture, the cartilage should be resected by punch (1.5-2mm) to induce granulation tissue from the soft tissue on the opposite side, or the punching should be immediately followed by skin graft directly to the defect.
• Find the anatomical structures of the ear and their names in the diagram below(Figure 3).
- Helix, Antehelix, Scaphoid Fossa, Triangular Fossa, Crus of Helix, Tragus, Antitragus, Concha, Symba.
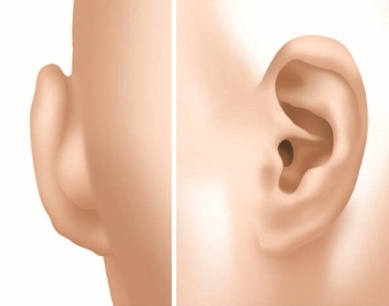
Figure 3. Diagram.
2. Things to be considered before surgical treatment of earlobe keloids
1) Conventional local treatments include intralesional injection of steroid, bleomycin or 5-FU, silicone gel application or silicone pressure sheet, metal pressure earring such as magnets or splint and cryotherapy, which have limited effect on preventing recurrence.
2) Simple excision followed by pressure has been reported as successful in some cases, although there are few reports on long-term follow-up results. Simple surgical removal is not currently recommended due to high risks of recurrence and exacerbation, but intralesional resection (core, subtotal or intramarginal excision) entails less recurrence.
3) Perioperative steroid injection and postoperative imiquimod application have been attempted to prevent postoperative recurrence, although these methods are not recognized as effective methods due to weak prevention effect.
4) Radiation therapy was found as the most effective method in comparative studies on various treatments.
5) Uncontrolled cases by conventional treatments or recurrent cases after surgery require radiation therapy and should be transferred to a hospital that provides one.
6) Radiation therapy is most effective and successful when performed 3 times consecutively (low-dose fractionated radiotherapy: 12Gy in three fractions) within 24 hours after surgery.
3. Surgical techniques for treatment of keloids
1) Intra-marginal or Subtotal Excision.
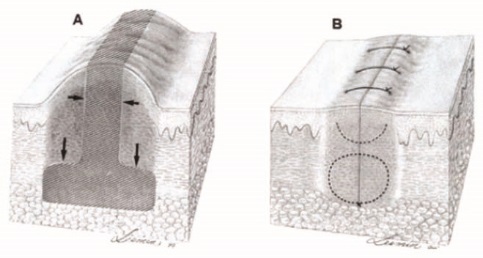
Figure 4. Intra-marginal Excision. JAAD 2002;47:307~9.
2) Core Excision with Supra-keloidal Flap.

Figure 5. Core Excision with Supra-keloidal Flap.
3) Preop TRA + Core Excision + RT.
4) My Current Approach: Summary.
4-6 weeks before surgery: Intralesional triamcinolone injection 20mg/ml/2 weeks.
Surgery: core excision with suprakelidal flap under local anesthesia
Radiation therapy within 2 hours after surgery: fractionated RT(12Gy in three fractions).
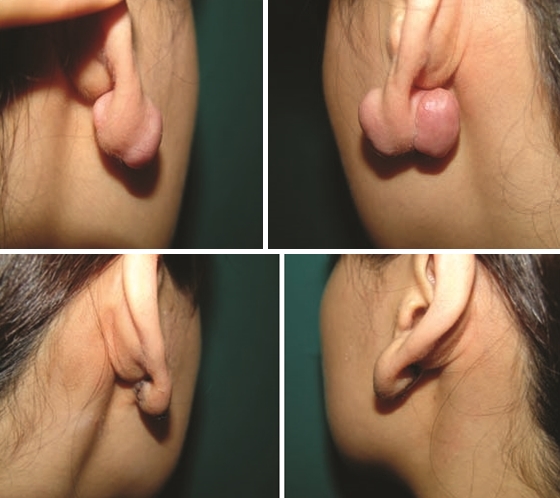
Figure 6. Preop TRA + Core Excision + RT.
References
1. Dinh Q, Veness M, Richards S. Role of adjuvant radiotherapy in recurrent earlobe keloids. Australas J Dermatol. 2004 Aug;45(3):162~6. Review.
2. Sclafani AP, Gordon L, Chadha M, Romo T 3rd. Prevention of earlobe keloid recurrence with postoperative corticosteroid injections versus radiation therapy: a randomized, prospective study and review of the literature. Dermatol Surg. 1996 Jun;22(6):569~74.
3. Field LM. Subtotal keloid excision–a preferable preventative regarding recurrence. Dermatol Surg. 2001 Mar;27(3):323~4.
4. Lee Y, Minn KW, Baek RM, Hong JJ (2001) A new surgical treatment of keloid: Keloid core excision. Ann Plast Surg 46:135–140.
5. Brian B. Adams, Hugh M. Gloster. Surgical Pearl: Excision with suprakeloidal flap and radiation therapy for keloids. J Am Acad Dermatol 2002;47:307-9.
6. Berman B, Villa A. Imiquimod 5% cream for keloid management’ Dermatol Surg. 2003 Oct;29(10):1050~1.
- To be countinued -
▶ Previous Artlcle : #2. Pigmented Basal Cell Carcinoma on the Face Mimicking a Nevus
▶ Next Artlcle : #4. New Treatments of Multiple Cutaneous Neurofibromatosis
























