







Changes in Pain Severity and HRQoLOverTime
Overall pain and discomfort improved over time regardless of existence of chronic pain. However, the severity of pain and discomfort shown on EQ-5D was higher in a group experiencing current pain. The EQ-5D values improved over time in all groups but stayed lower in patients with current pain.
The role of burn- and individual-related factors in post-burn pain
Burn related factors that impacted pain were TBSA, TBSA-FT, and LOS. Gender, age, time from sustaining burn, and exposed area were found to be unrelated to pain.
Table 1 presents various individual-related factors that can influence pain. At the12 months follow-up, EQ-5D index, EQ-5D VAS, and IES-R were significantly associated with post-burn pain. History of mental illness and working were not associated with post burn pain.
.png)
Table 1.Severity of pain and its interference with general activities asassessed by the Brief Pain Inventory-Short Form in the 20patients thatreported pain at 2~7years after the burn.
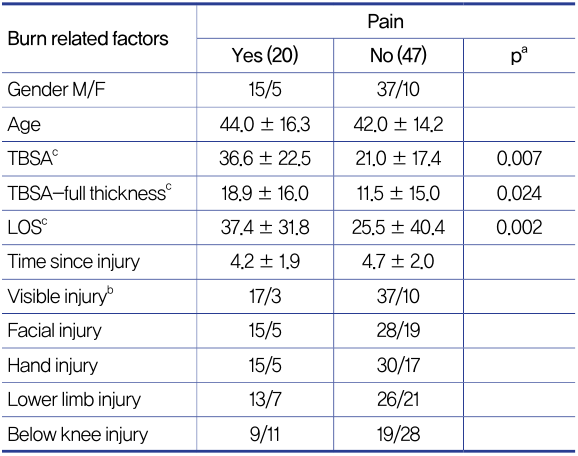
Table 2.Burn-related factors and the presence of postburn pain.
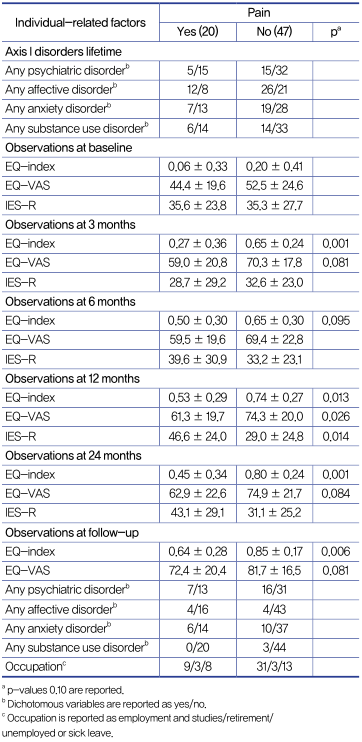
Table3.Total Body Surface Area(TBSA).

[Advertisement] PICOCARE - Manufacturer: WONTECH(www.wtlaser.com)
Discussion
The BPI-SF results show that a third of patients reporting early burn pain still experienced pain 2-7 years after (4.6±1.9 years). Pain severity and interference on daily life ranged from mild to moderate and two scales were highly correlated. Patients who had low HRQoL at 3 months were likely to report pain 2-7 years later. This is a very meaningful finding.
Patients were divided into two groups based on existence of current pain (BPI-SF) and changes in pain severity over time was assessed usingEQ-5D (pain·discomfort index). During the acute pain phase where pain is severe, there was little difference inpain severity between two groups. However, patients with current pain had higher pain/discomfort level at all follow-up points. The pain·discomfort index decreased with time but the index was drastically lower in the group with no current pain. At 12 months, patients with current pain showed marked change in their pain severity and this was the same from 24 months up to 7 years. This suggests that presence of pain at 12 months can predict the presence and persistence of pain later (2-7 years).
Many burn patients suffer from PTSD. Some fully recover but most progress into chronic PTSD and require continuous treatment of the residual symptoms. PTSD is known to impact the pain threshold. This study also showed that patients with currentpain had a high IES-R score at 12 months. This is encouraging as it could potentially be a predictor of increased post-burn pain severity at 12 months. The IES-R score at 12 months can be regarded as an independent predictor of pain in the future.
In agreement with the findings of Browne et al., this study also found that patients with chronicpost-burnpainhad extensive TBSA and longer LOS. In all follow-ups excluding the first three months, LOS was an independent predictor of chronicpost-burnpain. Additionally, LOS was an indirect marker of burn severity and complexity. Large TBSA, deepburn, number of surgeries, and infection, etc. were factors that influenced LOSand as such, they possibly had indirect impact on chronicpost-burnpain.
The pain severity andHRQoL were inversely correlated in both patients with and without current pain, with lower the pain·discomfort index correlating with higher theHRQoLscores. However, patients with current pain had a much lowerHRQoLscore. Therefore, EQ-5D can be a simple and useful method of evaluatingHRQoL in pain prevention.
-To be continued
























