







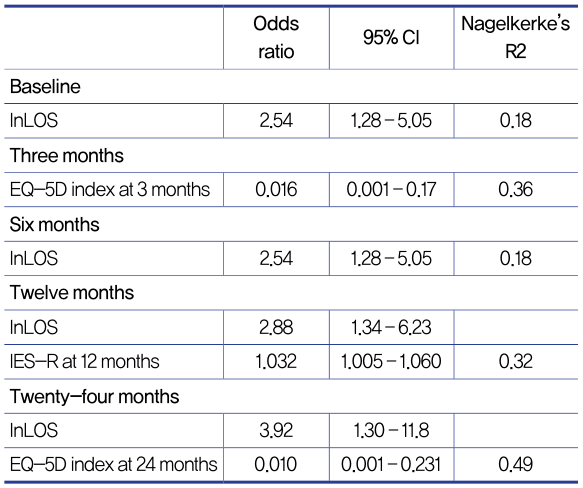
Table 4. Best fit regression models for prediction of the outcome variable painat various times after the burn.
The EQ-5D index at three months was found to be an independent marker of changes in pain over time. HRQoLat 24 months is also an independent marker of persisting post-burn pain.Therefore, it can be said that pain andHRQoL are correlated.
BPI-SF and EQ-5D had little correlation.All of the patients who reported pain on BPI-SFalso reported pain and discomfort on EQ-5D. On the other hand, many of the patients who reportedpain on EQ-5Dsaid they did not experience pain on BPI-SF. This may be due to the fact that BPI-SF focuses on specific pain such as cancer or burn pain and EQ-5D includes non-specific pain and discomfort.
Conclusion
Chronicpost-burnpain causes stress to patients and lowersHRQoL. HRQoL at the early phase of burn can be used as a predictor ofchronicpost-burnpain and as a useful marker in burn-related pain treatments.
*Health-related quality (EQ-5D) early after injury predicts long–term pain after burn (Burns. 2016 Dec;42(8):1781-1788. doi: 10.1016/j.burns.2016.05.016. Epub 2016 Jun 21)

[Advertisement] Reandnè Thread Series – Manufacturer: GTG KOREA(www.gtgkorea.co.kr)
The Association Between Healing Time And The Incidence Of Hypertrophic Scarring In Pediatricscalding Burns
Background
It is well known that the risk of hypertrophic scar rises with deeper burns and longer treatment duration. Today’s burn care uses wound dressing that promotes an ideal wound conditionor early excision and graft in deep burnsto minimize the treatment duration and speed up recover. However, it is difficult to accurately assess the depth of the burn and this requires and a lot of experienceon the part of the doctor. Efforts are being made to more accurately assess the burn depth using laser Doppler, infrared thermography, or spectrophotometric intracutaneous analysis, etc.
There are three approaches to scalding burn treatment. First is early excision and graft for promoting quick wound closure by removing dead tissues in the early phase. Second is dermal preservation strategies where silver containing topical cream is used for wound dressing. Third is initial conservative treatment with delayed grafting where 2-3 weeks of treatment is followed by grafting in the shrunken wound.
In 1983, Deitch reported that scalding burns that heal within 14 days carry a low risk ofhypertrophic scar and those that take between 14 to 21 days to heal have 1/3 chance of developing into hypertrophic scars. This indicates that scalding burns that remain after 21 days can only be addressed by surgery for preventing scarring. In 2006, Cubison found similar results in pediatric scalding burns. However, there is paucity of data on how hypertrophic scars impact the patient’s finances and quality of life. Some patients require reconstructive surgery for functional and aesthetic improvement.
Recent development and use of silver-containing wound dressing materials have contributed to shorter treatment period and decreased the need for surgery. We performed a restrospective study to examine the following two associations in pediatric patients with scalding burns who were treated with silver-containing dressing materials with the follow-up of 5 years.
1. Relationship between treatment period and the incidence of hypertrophic scar in pediatric scalding burns
2. Impact of skin graft, mechanism of injury, and site on the incidence ofhypertrophic scar
























