







None of the 20 patients who sustained scalding burns on the face and neck developedhypertrophic scar. The upper limbs and body had a higher incidence ofhypertrophic scarring and a longer treatment period(mean 16.7 and 15.6 days respectively, p < 0.01). When upper limbs were divided into shoulder and arm, the mean treatment period was 19.5 days in the shoulder and 19.8 days in the arm( p = 0.02).
The incidence of hypertrophic scars was the highest with the burn causes of hot water(18.8%), tea(15.5%), other liquids(17.2%) however, no significant differences were found among these causes in terms of the incidence(Table 3).
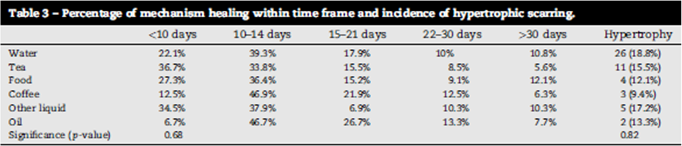
Table 3. Percentage of mechanism healing within time frame and incidence of hypertrophic scarring.
Discussion
The purpose of burn care is to shorten the treatment period and minimize scarring by reducing infection and morbidity. The primary objective of this study was to identify a correlation between the treatment period and the incidence of hypertrophic scar in pediatricscalding burns and a significant correlation was found between the two. However, the overall incidence of hypertrophic scar was lower than what was previously reported(16.1% vs. 35%, Table 4). This may be due to the use of silver-containing dressing materials.

Table 4. Healing time compared between studies.
The secondary objective of this studywas to examine the correlation between the incidence of hypertrophic scarand skin graft, mechanism of injury, and burn site. One noticeable finding of this study was that delayed excision and graft could not prevent hypertrophic scarring. Although not statistically significant, among patients with 22-30 days of treatment period, those given conservative treatment had a lower rate of hypertrophic scarring compared to those receiving skin graft(80% vs. 56.5%, p = 0.26). This was similar in patients with a treatment period of 30 days or more(85.7% vs. 81.3%, p = 1). Therefore, I believe that surgery is more effective in scalding burn and extra efforts are required for optimal results. I believe the ideal approach is to correctly assess the burn depth and carrying out the surgery in the early phase. At later phases, only carry out surgery carefully considering the risk of general anesthesia and donor site morbidity and if secondary healing is possible.
However, as for patients with severe and deep burns who received skin graft, it was difficult to obtain clear information on the burn depth due to the retrospective nature of this study. In addition, objective scar assessment tools such as Vancouver Scar Scale were not used, which may limit the validity of the findings.

[Advertisement] FCR® (Fractional Prickle CoralCalcium Regentron) – Manufacturer: (www.illglobal.com)]
Imaging such as laser Doppler can be an effective method of assessing burn depth. The part of the wound requiring skin graft and the part that can heal with conservative therapy within 15 days show different tissue perfusion at 3-5 days. This can be used to effectively carry out early excision and graft.
Previous studies reported the following risk factors of hypertrophic scar in burn care; infection, women, neck and upper limb, repeated surgery, meshed skin graft, dark skin, skin tension, and younger age, etc. As for the burn sites, the torso and upper limbs were found to be more susceptible to hypertrophic scarring. Therefore, early extension and graft or scar prevention treatments whould be considered in scalding burns on the torso and upper limbs. Areas such as the shoulder, arm and torso which have a higher risk of hypertrophic scarring are often covered by clothing. Not removing the clothes immediately after hot liquid is spilled increases exposure time to the hot liquid and may increase the risk of hypertrophic scarring. However, if the clothing is thick enough or is water-proof material, it can protect the skin against hot liquid. More research is needed in this regard.
As for the mechanism of injury, the incidence of hypertrophic scars was the highest in patients sustained the burn from boiling water. Boiling water has a higher temperature than the lukewarm tea or coffee. I believe the most important factor that impacts the burn depth is the temperature and a hotter liquid is more likely to cause deeper burns and hypertrophic scars.
Conclusion
This study showed that there is a clear correlation between the incidence of hypertrophic scar and scalding burn treatment period. Despite its high cost, the silver-containing dressing material effectively shortened the treatment period compared to previous studies. It is noteworthy that the treatment period was proportionally correlated with the risk of hypertrophic scarring, regardless of the type of treatment used. It is also interesting that the incidence of hypertrophic scarring was higher with delayed excision and graft. I believe using a more precise imaging tool than laser Doppler to assess burn depth as well ascarrying out early excision and graft within 3 weeks would be an effective approach in scalding burns. More research is needed in this regard.
* This article was cites information from BURNS, p. 5.9-513 of Volume 43, 2017.
-To be continued
























