








▶ Previous Artlcle : #11-2. Biological Dressing Ⅱ
Glycerol Preserved Allograf; GPA
·GPA replaces about 85% of water content of the skin with glycerol and maintains the structural stability necessary for allogeneic transplantation.
·GPA is advantageous in that it can be stored for at least two years longer than CPA, has antibacterial, antiviral characteristics and causes less immune response compared to CPA. However, the vital structure of allograft is partially destroyed which in turn compromises graft survival.
[Advertisement] ULTRA THIN WALL NEEDLE – Manufacturer: AESPIO(www.aespio.com)
Human allograft, the most effective care of patients with severe burns, is an important procedure that supports the effectiveness of biological dressing and the concept of ‘early excision and graft’ which has become the gold standard of burn care (Fig 3-5).
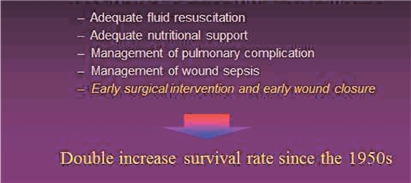
Fig 3. Sugical wound closure increases burn survival rates.
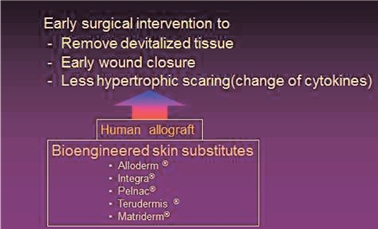
Fig 4. Early excision & graft.
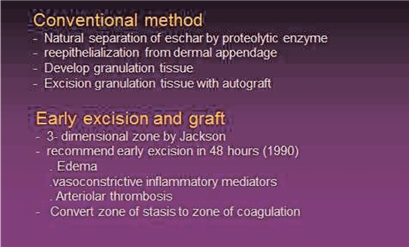
Fig 5. Conventional method vs. Early excision and graft.
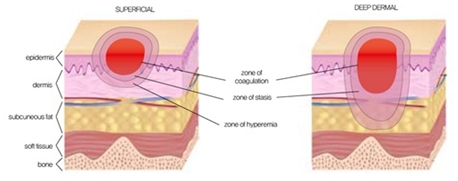
Fig 6. Three-dimensional Zone Theory.
The survival rate of patients with extensive burns has at least doubled in the last 50 years. This is thanks to various new developments in the field of burn care that reduce the incidence of sepsis such as effective fluid resuscitation, provision of sufficient nutrition to the patient, recognition of and better treatment for inhalation burn care, and introduction of various topical treatments (Silvadone, Sulfamylon etc.). However, the most prominent advancement in burn care would be introduction of ‘early wound closure, early graft’ which removes necrotic tissues and covers the wound as early as possible after burn injury.
The purpose of early excision of burn wound is to remove harmful free radicals, toxic substances and infection source by excision and provide early closure of the wound site. This reduces the likelihood of hypertrophic scar and minimizes severe late deformities of burn wound contracture. Development of various artificial dermis (AlloDerm, Integra, Terudermis, Pelnac, Matriderm etc.) and systemic management of donated human cadaver tissues in skin banks have greatly contributed to advances in the early excision method.
The traditional burn care methods still practiced are passive approaches that wait for the natural eschar separation by proteolytic enzymes in the skin. Here, epithelization is left to the action of remaining skin appendages after crust removal or much time is spent on waiting for formulation of granulation tissues in the wound bed for delayed skin grafting. On the contrary, the recent development in burn care that uses more active approaches is based on the Three-dimensional Zone Theory (Fig 6) proposed by Jackson. In short, dead tissues are quickly removed within 48 hours of sustaining burn injury while vasoconstrictive inflammatory mediators are still in action and before edema sets in. This prevents the irreversible transition from the zone of stasis to zone of coagulation.

Third degree burn in the chest from flames. Three days after burn injury. After escharectomy, the wound was covered with Glycerol Preserved Allograft (GPA). Two weeks after allograft. Granulation tissues are formed in the wound bed and parts of allograft are still visible. Remaining allograft can be removed during autograft procedure.

1:4 mesh autograft was performed over the granulation tissue. In some cases, Cultured Epithelial Homograft (CEH) or Cultured Epithelial Autograft (CEA) are applied in a sandwich technique in over 1:4 mesh autograft to increase graft survival and accelerate healing process. Most of the wound was healed 3 weeks after mesh autograft.
-To be continued-
▶ Next Artlcle : #13-1. Non-allograft Biological Dressing Materials
























