








▶ Previous Artlcle : #13-2. Non-allograft Biological Dressing Materials
Autologous skin grafts
Types of Grafts
I. Split Thickness Skin Graft (STSG)
In a split thickness skin graft, the top layer of dermis, the epidermis, is harvested using a dermatome or skin graft knife and transplanted. This method allows for extensive wound coverage, and is the most effective and timely method for treating burn or trauma wounds due to its high graft survival rate.

[Advertisement] Ultra Skin/Pastelle – Manufacturer: WONTECH(www.wtlaser.com)
However, this method is liable to leave wide pigmentation lesions as well as uneven scars at the donor site. Compared to full thickness skin grafts (FTSG), engrafted sites for split thickness may have reduced elasticity as well as unsightliness and irregularities. Close attention should be given to skin color, texture, and elasticity when performing reconstructive surgery for correction of burn contractures or for frequently exposed areas of the body such as the face.
Recent trends have favored medium graft thicknesses ranging from 10~12/1000 inches. However, for better aesthetic outcomes in terms of color and texture of skin, 15~18/1000 inches is preferable. Because severe hypertrophic or unsightly scars could develop at the donor site, donor sites should be selected amongst clothed areas such as the buttocks or from the less scar-prone area of the back, with thicker skin (Fig 1).
The latest developments in bioengineered dermal substitutes act to supplement the natural dermis to minimize graft contracture. Therefore, harvesting a very thin layer of 5~6/1000 inches in thickness can bring outcomes comparable to STSGs of medium thickness, reducing aesthetic problems for the donor site (Fig 2). This method is especially beneficial for children predisposed to hypertrophic scars or elderly patients with very thin skin and prolonged healing time at the donor site.
An STSG greatly affects contracture, pigmentation, and texture of the surgical area depending on the thickness of its harvested graft. As patients want to avoid scarring as much as possible, doctors have to be particularly cautious of donor site morbidity. Therefore, close attention should be paid to factors such as the thickness of the harvested skin, the condition of the donor site, the area and shape of the region to be covered, etc. in the procedure.

Fig 1. The left image shows thick hypertrophic scars in the donor site harvested in the thickness of 12/1000 inches (thickness of regular skin graft).
The donor site of very thin grafts (5/1000 inches) harvested for dermal substitutes suffers much less scarring.
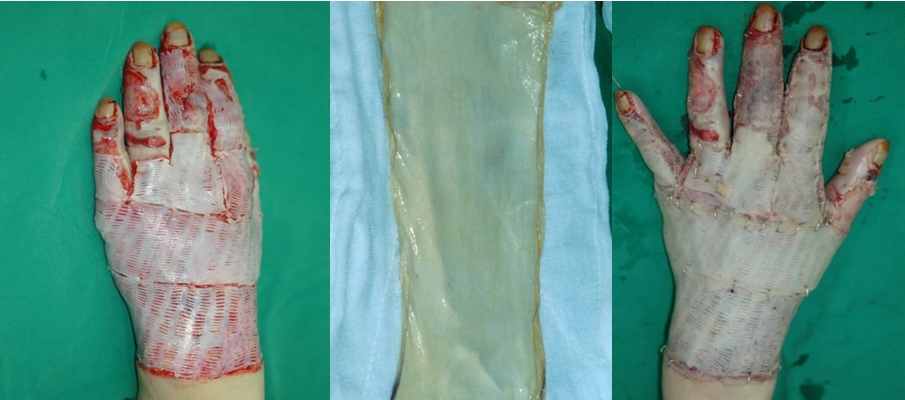
Fig 2-1. Treatment of a third degree burn using dermal substitutes.
The dermis is supplemented with a dermal substitute and very thin split-thickness graft (5/1000 inches) is carried out for hand function recovery and aesthetic outcome.

Fig 2-2. Images taken 1 year after the surgery show recovery of hand functions and good aesthetic outcome.
-To be continued-
▶ Next Artlcle : #14-2. Surgical Wound Coverage
























