








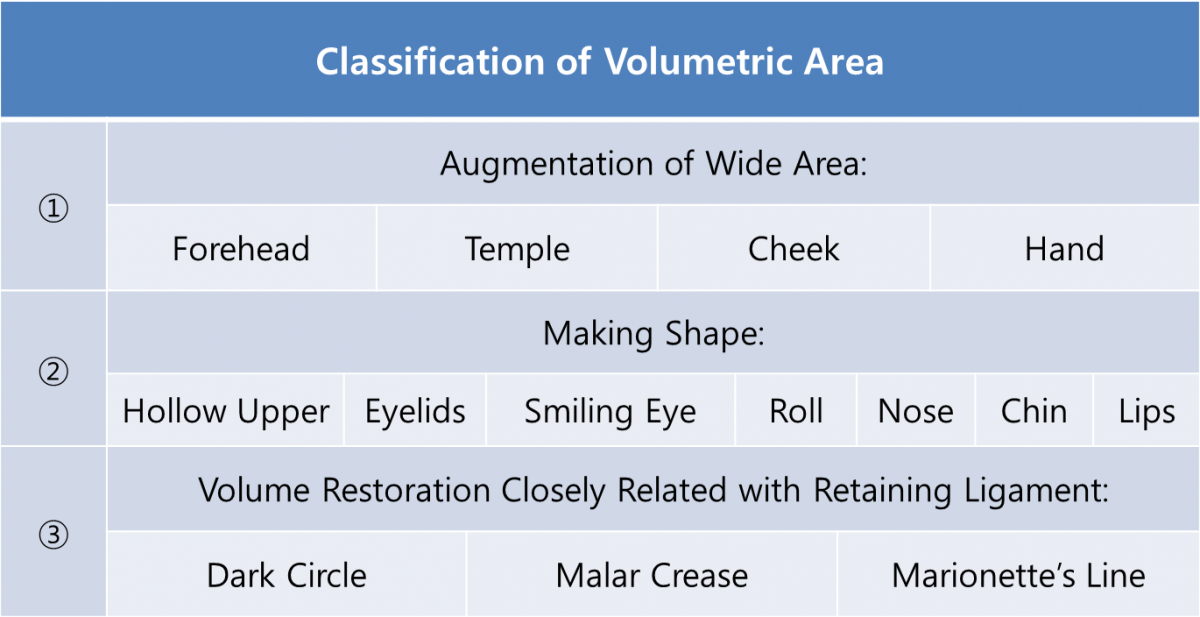
Table 1. Classification of dermal filler procedures.
In this article, we will discuss 'Volume Restoration Closely Related with Retaining Ligament', one of three basic dermal filler procedures; Augmentation of Wide Area, Making Shape, and Volume Restoration Closely Related with Retaining Ligament.
.png)
Image 1. Dark circles, malar creases, nasolabial folds (NLF)
Difficult areas
“Volume Restoration Closely Related with Retaining Ligament” can be applied to dark circles (tear trough), malar creases, NLF, and Marionette lines, etc. These areas pose a greater challenge than others (hollow upper eyelids, smiling, eye roll, nose, chin, and lips, etc.) where the aim is to create a new shape or spread the filler over a flat surface. Dark circles, malar creases, NLF, and marionette lines have different dynamics due to the involvement of the retaining ligament. It is particularly important to accurately understand the dynamic structure of each area.
In these areas, the retaining ligaments pull on the skin and create under-eye bags or nasolabial folds. Therefore, one should be able to locate where the retaining ligament attaches to the skin and the strength of the pull. The dynamics of the retaining ligament and the skin can be compared to that of a suspension bridge. Such dynamics have to do with the sagging and indentations of the aging skin. The structure of the retaining ligament and the attached skin is quite complicated and requires more skills than simple shaping or volumizing techniques.

[Advertisement] FCR® (Fractional Prickle CoralCalcium Regentron) – Manufacturer: (www.illglobal.com)]
Dark circles are pulled by the tear trough ligament, orbicularis retaining ligaments and malar creases by the zygomatic ligament. Nasolabial folds are also affected by the retaining ligament. As the skin ages, the retaining ligament loses tension more slowly and does not sag in tandem with other tissues. This in turn causes discrepancies in location of tissues leading to lumps or indentations. The dermal filler procedure should fill the indented area and create superficial shape for optimal results. Visible improvement will not be achieved only with filling the indented area.
Therefore, it is important to inject the filler not only into the depth of the indentation but on the surface as well. Think of the technique as layering the filler material from the very bottom of the indentation up to the very surface of the skin, while being mindful of the retaining ligament pulling on the surface. The key is to address both the depth of the indentation as well as the surface shapes.
-To be continued
























