








▶ Previous Artlcle : AGNES reduces recurrence of acne by selective destruction of sebaceous glands Ⅰ
In theory, all follicles with sebaceous glands are susceptible to acne. However, patients presenting acne do not have acne developing from all follicles. Especially, recurring acne tends to return to the same follicle and is more likely to result in scars. I explain this phenomenon of acne recurring in the same follicle with ‘acne prone follicle theory’. This phenomenon (recurrence of acne in the same follicles) is caused by inflammation leading to microfibrosis (scarring) of pore walls and follicles. When male hormones stimulate sebaceous glands, follicles with fibrosis are more easily blocked compared to normal follicles. In short, not all sebaceous glands should be destroyed to treat acne. Repeated treatment on follicles currently affected by acne can cure acne prone follicles. The reason for the need of multiple treatments is that acne does not develop from all acne prone follicles simultaneously. From my clinical experience, most of the patients treated with selective destruction of sebaceous glands on current acne sites without affecting normal sebaceous glands did not experience recurring acne. This is in agreement with the report by Jin W. Lee et al. (Figure 3). Destruction of only sebaceous glands currently affected with acne based on the acne prone follicle theory can largely prevent recurrence.
[Advertisement] ULTRA THIN WALL NEEDLE – Manufacturer: AESPIO(www.aespio.com)
In PDT procedure, ALA is absorbed into follicles and light beams are irradiated. This damages sebaceous glands of all follicles. PDT damages surrounding healthy tissues for treatment of acne. It also does not completely destroy sebaceous glands which results in sebaceous gland recovery and subsequent acne recurrence. On the other hand, AGNES does not destroy sebaceous glands of all follicles, because it is simply not necessary to do so.
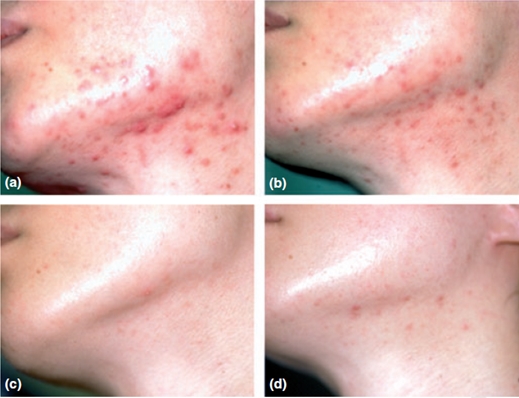
Figure 3. A 23-year-old man (a) before the initiation of treatment, (b) 1 month after the first treatment, (c) 1 month after the final treatment, and (d) 1 year after the last treatment. (Jin W. Lee et al).
One may be concerned about skin drying after sebaceous gland destruction. However, selective destruction of acne prone follicles causes negligible dryness. Removal of only hundreds of sebaceous glands among millions in the facial skin does not dry the skin. The most common side effect of selective destruction of sebaceous glands is burning. It would be a disaster to cause a burn in a patient visiting a dermatologist for improved aesthetic outcome. In the patient’s perspective, it is comparable to going out for wool and coming home shorn.
Burns are mainly caused by two factors; the carelessness of the performing doctor and damaged insulation of needles. The Japanese devices developed by Kobayashi et al. did not consider safety in the design. To identify existence of insulation breach during the procedure, the needle had to be removed from the handpiece and placed on a microscope. When the insulation was damaged during treatment, an experienced doctor can sense the skin is burning. This sensation may be similar to burning a wart or mole in bovie electrocautery. However, checking for insulation damage during treatment is burdensome and even when damage is suspected, the treatment is continued in most cases. Burning occurs when the insulation coating is breached. To prevent this, AGNES includes a device that easily checks insulation damage during treatment. The handpiece can be separated any time during treatment and the needles are magnified by 50 times on a screen for each checking of insulation damage. If damage is suspected, the needle can be quickly replaced which drastically reduces the risk of burn.
AGNES has a unique acne treatment process which differs from other methods. Unlike traditional acne treatments, AGNES is performed over two days. Destruction of sebaceous glands is carried out after acne extraction. The pre-procedure extraction empties the follicles and prepares them for AGNES treatment. If the follicle is filled with sebum, it dissipates the high frequency energy and thereby inhibits complete destruction of the sebaceous gland. All affected follicles are extracted to completely empty them before destruction of sebaceous glands is carried out.
The patient is instructed to visit the doctor on the following day of extraction and the debris from the previous extraction are removed again. The residual tissues of destroyed sebaceous glands and exudate coagulate to appear as crusts. Heating these crusts with a melting handpiece (Bipolar) soften and melt hardened crusts, making extraction very easy and less painful. The high frequency energy also has collagen remodeling effect which helps scar-free healing. If the second day’s procedure is not carried out, the coagulated crusts may become an infection source and recurring inflammation in the same spot brings scars. Therefore, it is necessary to make patients understand the importance of the second day procedure.
Another unique characteristic of destruction of selective sebaceous glands with AGNES is the number and interval of procedures. Unlike traditional acne treatments, AGNES does not require frequent or extensive treatments. Based on my clinical experience, about three procedures are sufficient to maintain the effect for two years. The treatment interval is about 1-2 months, between the first and second procedure. The third treatment can be performed months later when acne has recurred. Considering the cost, frequency and pain of acne treatments over many years, AGNES offers the most effective and cost-efficient treatment modality.
The key benefit of micro-insulated needles of AGNES is the protection of the epidermis. Despite its invasiveness, it does not involve downtime just like a non-invasive treatment. In other words, it offers the benefit of an invasive procedure while minimizing its disadvantage. Applying these principles, indications of AGNES can be widened beyond acne. Another key indication of AGNES is syringoma. Syringoma has been treated with CO2, Erbium lasers or chemical peeling, etc. However, the post-procedure epidermal loss results in long-term erythema and downtime. Also, multiple procedures should be repeated to bring effect in many cases. However, Shi-hyung Cho et al. have reported on successful treatment of syringoma with high frequency micro-insulated needles without downtime. This benefit is similar in AGNES as well. The needles currently used for acne are specified for sebaceous glands and may not be suitable in treatment of syringoma. However, if needles more appropriate for the depth and width of syringoma lesions are developed, better results can be expected. Under-eye fine wrinkles can also be addressed using the same principles. The dermis in this area is markedly thinner than other areas and the length and electricity levels of the needle should be adjusted accordingly.
A mild lifting procedure can be performed with the melting handpiece. As it uses bipolar energy the depth is limited but brings immediate lifting effect after procedure. It can be used in elasticity enhancement procedures.
-The end-
























