







Case
▶ Patient: 16-year-old male
▶ Chief complaint: Inflammation and edema repeated for several years around the big toenails
▶ Past medical history and family history: No particular past medical history or family history
▶ Skin findings: The patient had initially received gutter splint for repeated erythematous edema and swelling around left bilateral big toenail and right lateral big toenail and visited for curative surgery.
▶ Diagnosis: Moderate(Stage II) bilateral ingrown toenails
▶ Treatment: Despite gutter technique (see the picture and description below), the symptom was not completely relieved. For curative surgery, part of the nails were removed and the matrix by high-frequency electrocautery, after which the symptoms were fully recovered.

Figure 1. Repetitive inflammation and edema around the big toenails
Overview of Ingrown Toenail
1. Causes
First, the nail bed inflicts wound to the surrounding skin. Repetitive inflammation and infection from the foreign substance results in a lesion accompanying hypertrophic soft tissues around the nail with severe pain and malodorous exudate. It occurs most commonly around the big toenails, mainly due to cutting the nail rounded off at the edges or not in a straight line. Other causes include repetitive or careless injury, genetic susceptibility, hyperhidrosis and bad hygiene. Bad nail care, due to poor visibility or using the wrong instrument, leaves prickly nail, which grows so that it cuts into the soft tissues around the nail. The symptom is aggravated when the nail cuts deeper due to excessive activity, tight shoes or socks, and overweight or obesity. Anatomical shape (wide nail fold, thin and flat nail plate, etc.) has been suggested as a risk factor, but there is no supporting evidence. Leg edema from diabetes, obesity and thyroid, heart or renal disease may also increase the risk.

[Advertisement] MAGNUM(Q-switched Nd:YAG Laser) – Manufacturer: (www.i-dana.com)]
2. Symptoms
Patients are classified to 3 stages – mild, moderate or severe – depending on their symptoms. Mild symptoms entail swelling, erythema, edema and tenderness of nail fold. Moderate case has more severe edema, exudate, and symptoms of infection or ulcer. When the condition progresses to a severe case, it accompanies chronic inflammation, granuloma, and markedly hypertrophic soft tissue.
3. Treatment Algorithm by Symptom
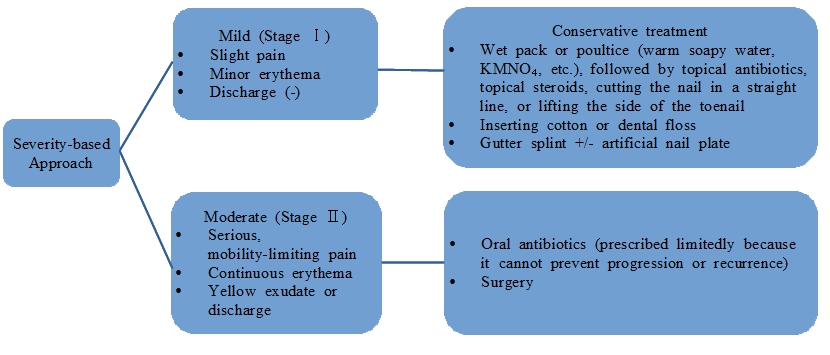
4. Treatments
Cases with severe pain, infection, nail deformation or chronic recurrent paronychia need treatments. If a patient is not amenable to surgery, allergic to local anesthesia, susceptible to hemorrhage or pregnant, conservative management should be attempted first before surgery. Patients requesting surgery should be informed of risks and benefits of conservative and surgical treatments as well as alternative treatments before making a decision.
1) Non-surgical, conservative treatments
Conservative treatment is a cost-effective and reasonable approach for mild or some of moderate cases without severe pain, erythema or infection, although it is limited by the need for repeated management every 2 week to 2 months on average. Below are the currently attempted methods:
① Soak the symptomatic foot for about 10-20 minutes in warm KMnO4 (1:15000), normal saline solution or soapy water, followed by application of topical antibiotics. The process is repeated for days until the symptoms are relieved.
② Put a small piece of cotton ball to the side of the ingrown nail and replace it repeatedly until the symptoms are relieved.
③ Several years ago, I have reported the method of inserting dental floss under the ingrown nail. This is an effective and simple method for relieving pain when there is no secondary inflammation.
④ Gutter splint (eg. An inserting tube is made from a sterilized vinyl IV fluid set or butterfly needle set. After completing the insertion, the site is fixed with a sticking plaster or instant glue.) (Figure 2)
⑤ Artificial nail: Plastic artificial nail is placed under the nail and fixed with instant glue.

Figure 2. Intraoperative (A) and postoperative (B-Left, C-Right) findings
2) Surgical treatments
Partial or complete removal of nail is attempted for ingrown nail with local infection. Destruction of matrix should be considered when the symptom is severe and recurrent. Phenol, high-frequency electrocautery and CO2 laser has been attempted in this case as effective alternatives. The most common method is to remove part of the nail, including the ingrown nail, and perform matricectomy using 80-88% phenol. In a Cochrane systematic review (including evidence-based medical research) comparing this method with direct removal of matrix, the two methods were comparable in efficacy but removal with phenol was more effective in terms of preventing symptom recurrence. Some studies reported that the risk of postoperative infection was slightly higher when phenol was used. However, it is known that preoperative application of topical antibiotics did not reduce the risk of recurrence or infection and phenol does not increase the risk of infection compared to surgery, although excess use of phenol may induce discharge lasting for several weeks, which could be reduced by swabbing 20% ferric-chloride for 20-30 seconds. When symptom is very severe, bilateral nails can be partially removed before conducting the above procedures. Matricectomy with CO2 laser induces less bleeding, has the effect of immediate sterilization, is less painful after the operation, and particularly causes less damage to the surrounding normal tissues. However, it is limited by the longer time it takes for reepithelization by second intention healing, requiring about 6 weeks of treatment, and the need for expensive equipment. The laser procedure can be performed completely and accurately by marking the nail matrix with methylene blue before the procedure.
3) Comparison between surgical and non-surgical treatments in Stage I and II: There are recent comparison studies that are helpful for determining how to treat patients visiting with ingrown nails. These studies compared efficacy, recurrence rate, postoperative infection, procedural time and postoperative disorders between surgical treatment (Winograd) and non-surgical treatment (Sleeve). The result of Winograd method can be different among operators, because it is highly affected by the operator’s experience. The Sleeve method is effective, simple, inexpensive, associated with less postoperative disorder, complication or recurrence, and allows for rapid return to normal activity, making it most appropriate as a first-line treatment in terms of high patient satisfaction and usefulness.
※ Winograd method – longitudinal incision, 2nd incision at nail fold, wedge removal of nail matrix, lateral nail fold, granulation tissue dressing.
※Sleeve (gutter) method – granuloma electrocautery, lateral ingrown nail removal, flexible tube insertion along the groove dressing
4) Complications
⓵ Recurrence due to incomplete removal.
⓶ Injury or infection of the surrounding tissues (fascia or periosteum) due to excessive cautery or resection.
⓷ Debridement, oral antibiotics or X-ray assay is needed when the lesion is not recovered in weeks.
References
Rounding C, Bloomfield S. Surgical treatments for ingrowing toenails. Cochrane Database Syst Rev. 2005;(2):CD001541.
Aksakal AB, Atahan C, Oztas P, Oruk S. Minimizing postoperative drainage with 20% ferric chloride after chemical matricectomy with phenol. Dermatol Surg. 2001;27(2):158-160.
Woo SH, Kim IH. Surgical pearl: nail edge separation with dental floss for ingrown toenails. J Am Acad Dermatol. 2004;50(6):939-940.
Arai H, Arai T, Nakajima H, Haneke E. Formable acrylic treatment for ingrowing nail with gutter splint and sculptured nail. Int J Dermatol. 2004;43(10):759-765.
Gerritsma-Bleeker CL, Klaase JM, et al. Partial matrix excision or segmental phenolization for ingrowing toenails. Arch Surg. 2002;137(3):320-325.
Zuber TJ. Ingrown toenail removal. Am Fam Physician. 2002;65(12):2547-2552, 2554.
Monheit GD. Nail surgery. Dermatol Clin. 1985;3(3):521-530.
Brown FC. Chemocautery of ingrown toenails. J Dermatol Surg Oncol. 1981;7(4):331-333.
Ozawa T, Nose K, Harada T, et al. Patrial matricectomy with a CO2 laser for ingrown toenail after nail matrix staining. Dermatol Surg. 2005;31(3):302-305.
- To be continued -
▶ Previous Artlcle : #5. Removal of Multiple Lipomatosis
▶ Next Artlcle : #7. Pre-Surgical Knowledge for Preparation of Facial Tumorectomy in the Out-Patient
























