







Case
▶ Patient: A 41-year-old male
▶ Chief complaint: Multiple nodules and cysts palpable on the trunk and extremities for several years (Duration: occurred several years ago).
▶ Past medical history and family history: No remarkable past medical history or family history
▶ Skin findings: Various sizes of tender subcutaneous nodules and cysts of normal skin color are observed on the trunk and extremities (Figure 1).
▶ Diagnosis: Multiple lipomatosis
▶ Treatment: Incision-Pinch technique (Figure 2 and description below) were performed, after removal which the lesions were cured without recurrence.
▶ Histological findings: Covered by thin connective tissue membrane and composed of mature adipocytes inside.
▶ Histopathological findings of the lipoma (Figure 3): Mature adipocytes are aligned as a lobule and mostly covered by fibrous membrane. Although rare, lipoma without membrane infiltrates the muscular layer (infiltrating lipoma).
[Advertisement] ▶ Aileen plus(Long pulsed Nd:YAG Laser) – Manufacturer: FineMEC(www.finemec.net)
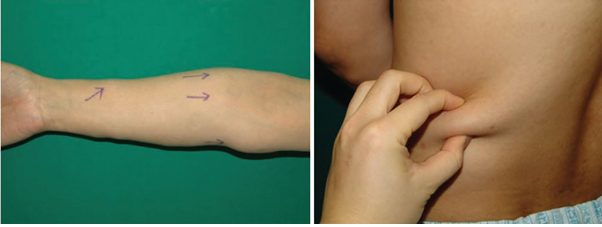
Figure 1. Multiple subcutaneous tender nodular cysts of various sizes
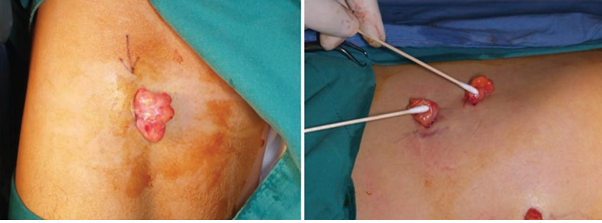
Figure 2. Lipomas sticking out of the skin by Incision-Pinch method. Lipomas 3-4 times bigger than the incision length can be removed.
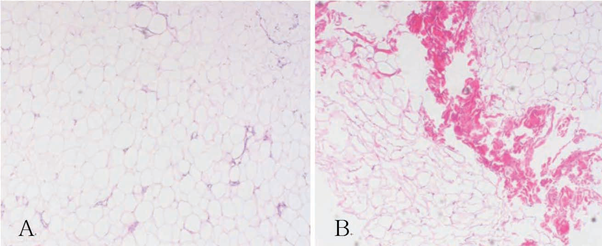
Figure 3. Histological findings (H&E, x40) before (A) and after (B) direct laser coagulation
Discussion of the Treatment of Multiple Lipomatosis
Currently Available Treatments
Nonsurgical Treatments
Nonsurgical treatments, including steroid injection (1-3ml, 10mg/ml, lesion size ≤1 inch), lipolysis by deoxycholate injection, laser lipolysis (Nd:YAG, Diode laser), liposuction (in cases where scar is an issue, 16G >canula), and lipolysis or liposuction by Tumescent anesthesia, are used for small lesions only.

Figure 4. After central incision inside the border of tumor (A). After detachment and slight pressure (B). After sufficient pressure (C).
Surgical Resection
Simple resection, punch-pinch method, and other various methods are used for complete removal of lipoma, after which the lesion is cured. Below is the detailed description of my incision-pinch technique procedure:
1. Palpate the lesion before the procedure to mark the borderline → Disinfection → Local anesthesia with 1-2% lidocaine → Incision of the skin in a spindle shape along the relaxed skin tension line from the center at the length smaller than (about 3/4) the cyst → Pull some of the subcutaneous tissue with vascular clamp
2. Detach the lipoma with scissors from the surrounding tissue being careful about blood vessels and nerves
3. Once the detachment is successful, the lipoma can be pushed out in a single lump with pressure only. See if there is hemorrhage and, if so, apply hemostasis.
4. After the removal, suture the (dead) space with 3-0 or 4-0 Vicryl. When the dead space is deep and hemostasis is incomplete, the blood or serous fluid may collect in the space, requiring drainage.
5. Suture the skin with 4-0 to 5-0 nylon, if necessary.
6. Apply compressive dressing to prevent hematoma after suturing.
7. Check the surgical site at Day 2 and Day 7 after the surgery, and remove the suture 2-3 weeks later depending on the site. Complications, including infection/cellulitis/fasciitis, ecchymosis, hematoma, surrounding nerve injury (dysesthesia, sensory paralysis , etc.), surrounding vascular injury, secondary permanent deformation, excessive scar accompanying aesthetic deformation or contracture, muscular injury or stimulation, fat, fat embolus, periostitis or osteomyelitis, and seroma, may develop after surgical resection.
Method I Use
1. Incision-Pinch Technique: for multiple, superficial lipomas of relatively small size
2. Incision-Laser lipolysis-Pinch Technique
Applying large pressure to a small hall for a giant lipoma may end up with hematoma, purpura or other complications, and lipomas that are difficult to extract may require additional incision, leaving a large incision line scar. I attempted, therefore, to make minimum incision (1-1.5cm for giant lipoma) and then applied 1444nm Nd:YAG (Accusculpt, Lutronic, Seoul, Korea) Laser to the center of the lipoma to dissolve and reduce the lipoma (see Figure 5), followed by detachment and extraction of remaining lipoma tissue and fibrous septa through the same incision. Compared to the surgical method, this method reduces the risk of purpura, hematoma and surgical scar, and it allows for complete extraction of tumor, which is impossible by nonsurgical method, enabling prevention of recurrence and confirmation of lipoma subtypes (angiolipoma, plemorphic lipoma, adenolipoma, etc) and malignancy (liposarcoma) by histology of the extracted lump.

Figure 5. Laser lipolysis. The infrared aiming beam enables the visualization of the procedure site. Palpable borderline should be marked before the procedure so that the degree of lipolysis could be adjusted and to confirm complete removal after the procedure.
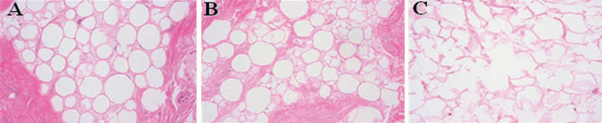
Results of lipolysis with 1444mm Nd:YAG Laser (H&E, x200) (A) 5J/cm² (B) 10J/cm² (C) 60J/cm²
Discussion on Lipoma Removal
1. Lipoma develops in every age group, but solitary type is detected more frequently among women, while multiple type is more frequent among men. Most cases are in their 40s to 60s. Some may develop congenitally in children, others after blunt trauma. These lipomas grow slowly, are asymptomatic and benign in most cases. Being asymptomatic, oval, movable cyst, lipoma can be diagnosed clinically by palpation, but it should be differentiated from epidermal cysts, other tumors of subcutaneous fat, nodular fasciitis, liposarcoma, metastatic cancer, nodular erythema, nodular subcutaneous fat necrosis, Weber-Christian subcutaneous panniculitis, vascular nodules, rheumatoid nodules, skin sarcoma, infection and hematoma.
2. Genetic multiple lipomatosis (Madelung’s disease, autosomal dominant inheritance, often develops symmetrically on the head and neck and the shoulder in men), adiposis dolorosa, Gardner’s syndrome (autosomal dominant inheritance, intestinal polyp, cyst, osteoma, etc.) occurs in rare cases. Variants include vascular lipoma, neomorphic lipoma, spindle cell lipoma and adenolipoma. It may develop in deeper body parts, such as muscle, abdominal organs, mouth and internal acoustic canal.
3. Lipomas are commonly removed for aesthetic reason, discomfort, paresthesia and other reasons. Most are small and singular, which can be well removed by Incision-Pinch method. Scar can be an issue for larger or multiple lipomas. Those larger than 4cm or with multiple lesions can be removed by liposuction, instead of resection. Lidocaine diluted to 0.05-0.5% is injected for Tumescent anesthesia and the cannula for liposuction is used as a curette to destroy fat lobule, which can be removed by negative pressure. Liposuction is associated with shorter procedure time, less scar, few side effects, superior aesthetic outcome, and the possibility of removing multiple lipomas through 1 hole. However, incomplete removal may lead to recurrence, and it is impossible to differentiate from possibly malignant liposarcoma. It is more assuring and effective, therefore, to use Incision-Laser Lipolysis-Pinch method that can minimize the incision, regardless of the size of multiple lipomas.
References
1. Christenson L, Patterson J, Davis D. Surgical pearl: use of the cutaneous punch for the removal of lipomas. J Am Acad Dermatol. 2000:42(4):675~6.
2. Hallock GG: Suction extraction of lipomas. Ann Plast Surg 1987: 18:517
3. Pinski KS, Roenigh HH: Liposuction of lipomas. Dermatol Clin 1990: 8:483
4. Rotunda AM, Ablon G, Kolodney MS. Lipomas treated with subcutaneous deoxycholate injections. J Am Acad Dermatol 2005: 53: 973~978.
5. Capriotti K, Humphreys TR. A novel technique for the extraction of Larger lipomas. Dermatol Surg 2009: 35: 493~495.
6. Goldman A,WollinaU. Lipoma treatment with a subdermal Nd:YAG Laser technique. Int J Dermatol 2009: 48: 1228~1232
7. Stebbins WG, Hanke CW, Petersen J. Novel method of minimally invasive removal of large lipoma after Laser lipolysis with 980 nm diode Laser. Dermatol Ther. 2011 Jan~Feb;24(1):125~30.
8. Pinski KS, Roenigk HH Jr. Liposuction of lipomas. Dermatol Clin. 1990 Jul;8(3):483~92.
9. SALAM GA. Lipoma Excision. Am Fam Physician. 2002. Mar.1;65(5):901~905.
- To be continued -
▶ Previous Artlcle : #4. New Treatments of Multiple Cutaneous Neurofibromatosis
▶ Next Artlcle : #6. Laser Treatment for Hemangioma and Vascular Malformation
























