







▶ Previous Artlcle : #2-1. The Etiology of Vitiligo: Autoimmune Theory and Neurohumoral Theory
4) Autologous cytotoxicity hypothesis. Environmentally exposed materials, such as phenols and quinones, and some of metabolites produced internally in the course of melanin synthesis are accumulated in the body, damaging melanocytes in people who are genetically sensitive to these materials. Chemical albinism is deemed to be caused by exposure to materials, which impairs the function of enzymes required for melanin synthesis. Tyrosine produces unstable byproducts during the synthesis of melanin, possibly damaging other cell matrices.
[Advertisement] ▶ Aileen plus(Long pulsed Nd:YAG Laser) – Manufacturer: FineMEC(www.finemec.net)
5) Biochemical theory. This theory explains the development of vitiligo by melanocyte toxicity, which is caused by abnormality of the biopterin pathway. (6R)-L-erythro 5,6,7,8 tertrahydrobiopterin (6BH4) and (7R)-L-erythro 5,6,7,8 tertahydropterin (7BH4) are all increased in vitiligo. 6BH4 is the essential cofactor of phenylalanine hydroxylase, an enzyme that converts orally consumed phenylalanine to tyrosine. When GTP-cyclohydrolase I, a synthetase of 6BH4, is hyperactivated or 6BH4 is increased by hypoactivation of 4a-hydroxy BH4 dehydratase, an enzyme that recycles 6BH4, the byproducts 7BH4 and H₂O₂ are accumulated through the metabolic pathway. Increased 7BH4 blocks out phenylalanine hydroxylases, additionally increasing 6BH4. High concentration of 6-biopterin is cytotoxic, leading to melanocyte damage.
6) Oxidative stress hypothesis. Catalse is aberrantly lower in both lesions and nonlesional areas of vitiligo patients compared to normal people. This is related to high H₂O₂ concentration in the whole epidermal layer. The exact reason is unknown yet, but it can be explained as follows: single nucleotide polymorphisms (SNPs) in the catalase gene may impair the combination and functioning of the enzyme subunits, particularly frequently in patients with vitiligo. Accumulated H₂O₂ diminishes the activity of catalase, and high cencentration of H₂O₂ is generated in the course of abnormal melanocyte synthesis where 6-biopterin is created. Moreover, increased norepinephrine and monoamine oxidase in vitiligo produces H₂O₂ as byproducts and reduces the activity of glutathione peroxidase. Calcium absorption disorder also may change the activity of thioredoxin/thioredoxin reductases.
7) Melanocytorrhagy hypothesis. This hypothesis proposes that vitiligo lesions are caused by migration or loss of melanocytes, which are weakly attached to the surroundings, by a slight friction or other stresses. This hypothesis can also explain Koebner phenomenon. In patients with non-segmental vitiligo, melanocyte separation can be observed 4-24 hours after applying a slight friction for 4 minutes on the normal skin. Tenascin present in extracellular matrix, which prevents melanocytes from attaching to fibronectin, was found to be increased in the skin of vitiligo patients, suggesting that melanocytes are lost quite easily and hardly redistributed to the lesion.
8) Reduced melanocyte survival hypothesis. This theory assumes that the the survival signal for melanocytes are reduced, causing melanocyte apoptosis. Keratinocyte-derived stem cell factors combine with receptor tyrosine kinase c-kit in the cell membrane to control the growth and survival of melanocytes. This is supported by reduced c-kit receptors in the margin of the lesion and reduced expression of stem cell factors around keratinocytes.
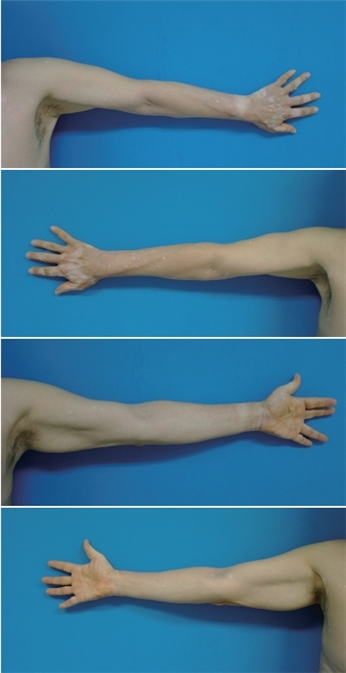
The above patient have had vitiligo, but not severe. From April this year, white spots appeared on the face and rapidly spread to the entire body. After PO steroid therapy combined with topical steroid, the symptoms have improved gradually. Blood test found T3/T4 reduced to 0.66/5.0 and ACTH to <1.0. Prolactin was increased to 16.4. Other findings were unremarkable.
-To be continued-
▶ Next Artlcle : #3-1. Diseases associated with clinical presentations
























