







Standards and requirements of basic facilities for performance of dermatologic surgery in the out-patient office
The American Academy of Dermatology (Refer to JAAD Guidelines of Care for Office Surgical Facilities) has categorized anesthesia into three levels as described in below, and presents detailed guidelines by classifying them into 4 areas (A. Facility requirements, B. Equipment requirements, C. Staff requirements, D. Procedure requirements) using the details by each level. Here at, the Class I Standards required for performing the surgery under topical anesthesia in the out-patient office is summarized as follows.

[Advertisement] ATLAS(Long pulse 532nm & 940nm dual wavelength) – Manufacturer: MEDRO(www.medro.net)
● Standards for Class I Facility: This class includes to topical, local and swabbing anesthesias only and rarely includes oral or intra-muscular administration of sedative or analgesic.
1) The building and offices to be used for hospital should be designed in conformity with the national standards for fire-fighting system, safety and sanitation.
2) The place should be equipped with appropriate hand-washing facilities and disposable towels .
3) The facility should be installed with appropriate surgical lighting system.
4) Emergency light system in preparation of black-out.
5) Air-conditioning system blocking incoming of insects or animals from outside through the air pathway.
6) Appropriate equipments required for topical anesthesia, surgical devices, operation table, monitor, and emergency resuscitation equipments
7) Furnishing with the fire-fighting safety equipments on which the periodic inspection tags are attached.
8) All staff related to the surgery should complete education of the basic emergency resuscitation technique. Also they should be educated how to prevent exposure to the blood-related infectious agent and to take necessary measures if being infected.
9) Safekeeping and control of medical records.
10) All staff should be familiarized with relevant statutes and shall be prepared for tactical actions against emergent situations.
Knowledge required for basic skills for excellent removal of tumor, good healing of wound and leaving the scar as small as possible
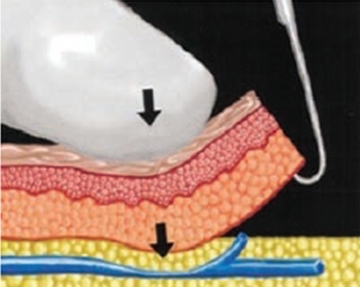
Figure 1. Effective Hemostasis Method. Pull the wounded site in use of skin hook and compress with fingers, then it is easy to accurately find the bleeding point and to perform hemostasis. JAAD 2002;47:938~9
1) Complete and effective hemostasis
Use of skin hook rather than tooth forceps (Figure 1): it is effective for hemostasis enabling to reduce the damage of wound and to find the point of bleeding easily (Use it together with a cotton swab)
● While performing the surgery, it should be ensured the complete hemostasis is done by using the methods described below additionally depending on the degree of bleeding and the size of blood vessel before closing the wound by stitches. (Table 1). The most effective hemostasis is to find the point of bleeding, and perform temporary hemostatis by compressing the bleeding point with a cotton swab(left hand) and apply the electrocautery (right hand) on the bleeding point only identified at instant detachment of the cotton swab. (Figure 4).
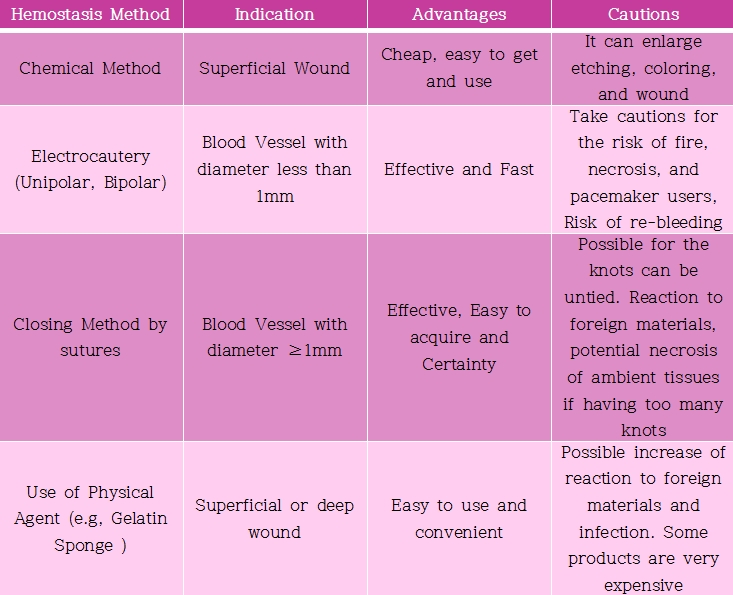
Table 1. Hemostasis Methods and Indications, Advantages as well as Cautions of each method
A) Mechanical/physical agents – Cotton swab and gauze in various size and number are used. the radio-frequency-utilized electrocoagulation is used most commonly
B) Chemical agents-Soak the cotton swab with Monsel’s solution (Fe) and Drysol (Al) and compress for about 20 seconds to 30 seconds to stop bleeding. Useful for simple biopsy or simple resection procedures .
C) Epinephrine gauze (Bossman gauze) – Use by soaking the blood from the wound during surgery
D) Physical agents (gelatin sponge) – Useful for prevention of post-operative hematoma.
● How to use cotton swabs: It is possible to absorb the bleeding, tract or stabilize the tissue by using cotton swab, Also it enables marking the tissue or testing the senses. Large Cotton Swabs-Applied with Antibacterial fluid, Useful for chemical peeling and sites with large amount bleeding. Standard Cotton Swabs is very useful for hemostasis and traction in the surgeries for orbital region and nasal area (Figure 2). Small Cotton Swabs-Useful for delicate tasks such as hair transplant or phenol cautery.

Figure 3. The magnifying glass-lenz are exchangeable by magnifying power. They are light weighted, inexpensive and convenient to use

Figure 4. Hemostatic Procedure during dissecting-Even when bleeding incurs while performing dissection, the assistant can secure the visual field using skin hook and suction, and the surgeon can clean the bleeding point with cotton swabs and perform hemostatis using electrocautery (JAAD 2002;47:938~9)
2) The process of performing tumorectomy and closing techniques
● The margin of tumor and the incision site should be designed using a marking pen in prior to remove the tumor.
● Depending on the location and the type of tumor, different approaches may be required, but the general principles are same.
● The surgeon should secure the visual field in use of a loupe (Figure 3) as possible in the process of performing the operation. In the incision process, only the surgeon uses the tooth forcep, and when traction is required and during the dissection process, skin hook is used. The surgical assistant must use the skin hook to reduce the damage of wound incurring during the hemostasis, traction and dissection process (Figure 4).
● Dissection (Undermining): The depths of dissection are varied by site and in case of face, it is performed as a subdermal procedure. Dissection should be conducted as directly looking at the surgical site and pulling gently to avoid damages to blood vessels and nerves. When bleeding is occurred, the point of bleeding should be found immediately for hemostasis (Figure 4), and cautions must be taken the dissection is to be progressed only to the extent that tension-free closing is possible depending on the tonicity, not to invade too deeply.
● Techniques of Closure: Appropriate wound closing technique is required to obtain good results in the aspect of aesthetics. Considering the functional and aesthetical outcomes for lesion, it is most important to minimize the tension applied to the wound. When ensured the suturing planes are in same height, making it eversion, and when taken extra cautions including performance of impact suture to reduce dead space, the possibility of the lesion's reopening or the possibility to have a scar is reduced. For this purpose, the closure stitching must be completed by closure of combining subcutaneous (fat layer), subdermal and superficial closure. When the lesion in size of 1~2cm, the dermal layer is being stitched for closure, using No. 5 or 6 absorbable suture making the knots are facing down, starting from the central part of defected part. Thereafter, the skin closure is to be conducted from the center in accordance with sequence from the rule of halves. In case of spindle shape defected lesion in the size of 2 to 4cm, the first stitching is performed by using No. 3 to No 5 absorbable sutures starting from the exact center of defected site, ensuring the knots are directed downward at subcutaneous layer, followed by the skin closure to be performed as aforementioned.

Figure 2. When cotton swabs are inserted into nostril and compress them upward, it can stabilize the rounded sides of the nose so that it makes hemostasis and stitching easy to perform
● Removal of suture and wound care (Table 2): It is possible to obtain aesthetically good result only when the sutures are removed using correct methods in timely manner depending on the presence/absence of tension by the site. Generally, it is desirable to perform the removal of sutures as soon as possible.
2) The complications likely to incur in connection to the pre-surgical knowledge for the types and prevention of surgery-related complications are varied from infection, delayed healing, hematoma, abscess of the sutured site, hypertrophied scar to Keloid. Each predisposition and method that should be aware of in order to prevent these complications are summarized and sorted out in Table 3
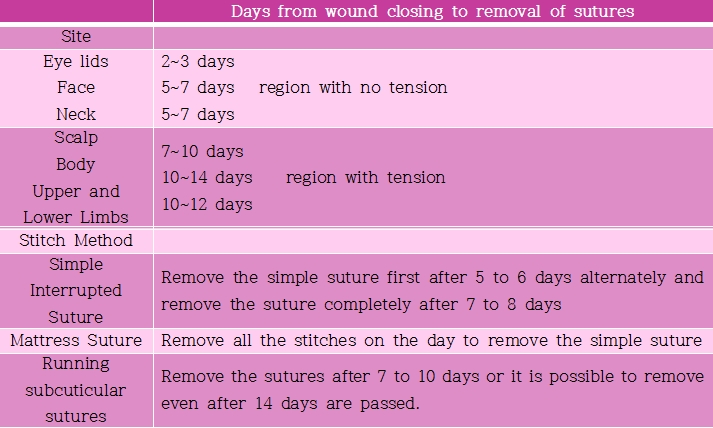
Table 2. Time to Remove the Suture by Site
References
1. Drake LA, Ceilley RI, Cornelison RL, et al. Guidelines of Care for Office Surgical Facilities. J Am Acad Dermatol. 1992;26:763~5.
2. Drake LA, Ceilley RI, Cornelison RL, et al. Guidelines of care for office surgical facilities. Part II. Self-assessment checklist. American Academy of Dermatology. J Am Acad Dermatol. 1995;33(2 Pt 1):265~70.
3. Robinson JK. Atlas of Cutaneous Surgery .Saunders .September 5, 1995.
4. Keyvan Nouri,,. Complications in dermatologic surgery Elsevier Health Sciences, 2008.
- To be continued -
▶ Previous Artlcle : #7. Pre-Surgical Knowledge for Preparation of Facial Tumorectomy in the Out-Patient
▶ Next Artlcle : #9-1. Surgical Treatment of Axillary Hyperhidrosis
























