








Male pattern Hair Loss affects about 50% of adults in western countries and about 15-20% of adults in Korea. In this condition, hair loss develops after adolescence and hair growth cycle, including the growth phase, becomes shorter than the cycle of the previous hair, gradually making hair thinner and ultimately resulting in suppressed hair growth. The most important factors of male pattern hair Loss are androgen and genetic background, the associations of which found in 1942 by Hamilton. He suggested that androgen in the presence of genetic background is the cause of hair Loss, considering the fact that the men who lack androgen due to castration before adolescence did not have hair Loss despite having genetic backgrounds, and that they developed hair Loss when androgen was administered and hair Loss stopped when the injection was discontinued. Therefore, the technical term for male pattern hair Loss is androgenetic alopecia from the combination of androgen and genetic. However, the terms male pattern hair loss and female pattern hair loss are more commonly used because the hair loss shows specific pattern for each sex (Figure 1).
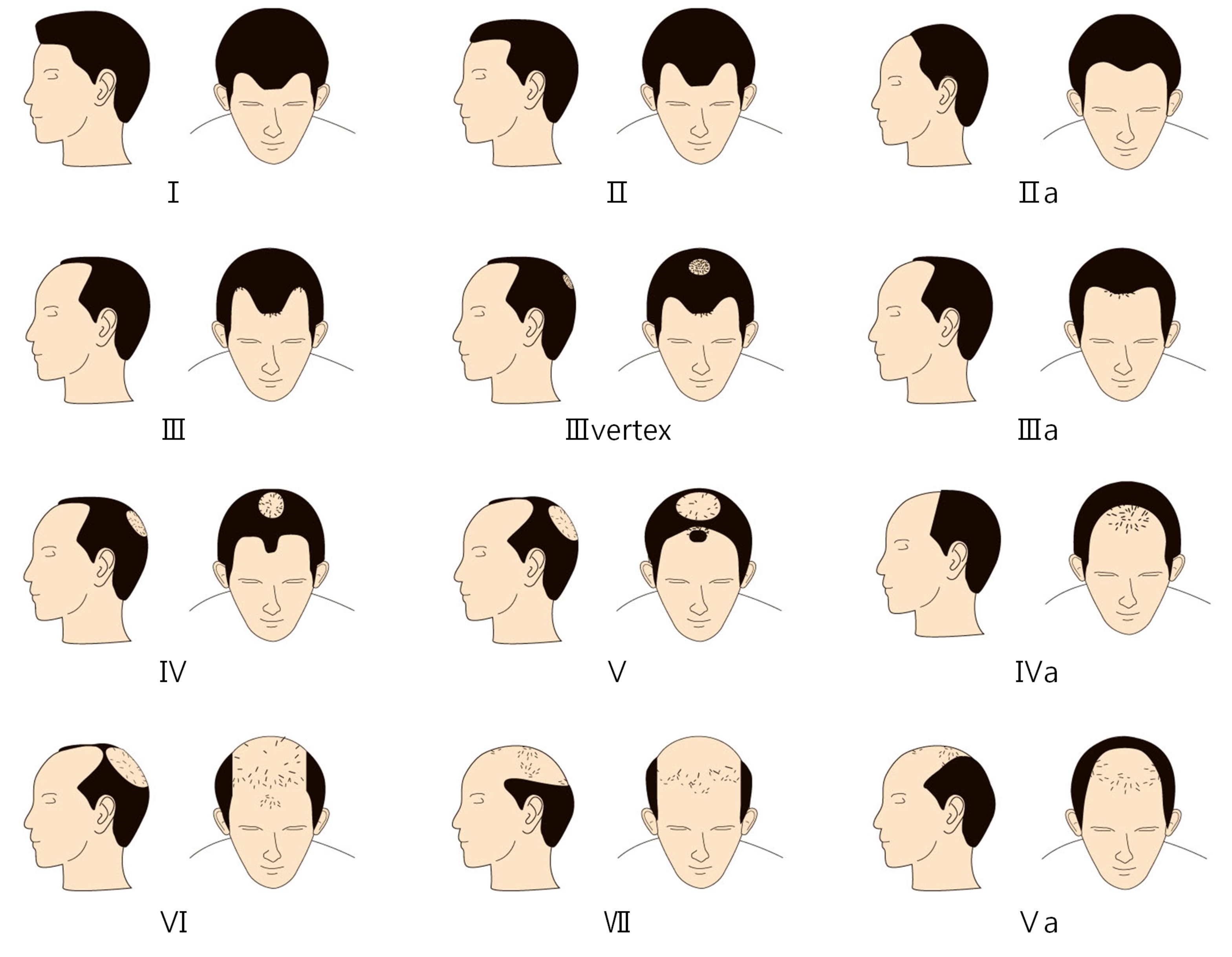
Figure 1. Classification of male pattern hair loss (Norwood Classification).
[Ad. ▶ ULTRA THIN WALL NEEDLE - Manufacturer: AESPIO(www.aespio.com)]
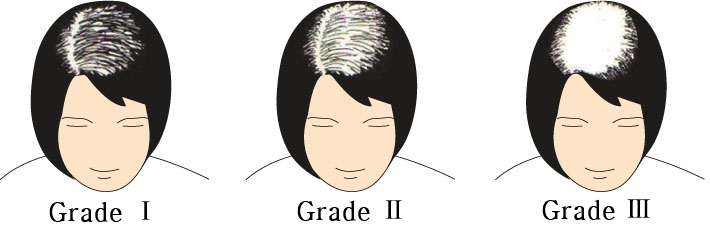
Figure 2. Classification of female pattern hair loss (Ludwig Classification)
In case of male pattern hair loss, after adolescence, testosterone becomes dihydrotestosterone (DHT) at the hair papilla where the activity of 5α-reductase is high, and DHT combines with androgen receptor, which is highly distributed on the area of hair loss, to reduce the production of growth factor, which stimulates the growth of hair matrix, or to inhibit hair growth by generating a factor that inhibits the growth of hair matrix. Female pattern hair loss is characterized by thin hair and reduced hair dense at the center of the head, while the hairline is preserved. The center region becomes larger while hair loss progresses. In this case, the hair loss develops gradually over several years, and the hair loss on top of the head becomes more widely distributed accordingly, revealing more scalp as the hair loss progresses. Unlike male pattern, female pattern hair loss does not result in complete baldhead but is characterized by slow progression of the disease, making it distinguishable from telogen effluvium, where hair falls off from the whole scalp mostly due to pregnancy or drugs.
Female pattern hair loss is known to increase in prevalence with aging, as with male pattern hair loss, and is commonly observed in post-menopausal women, although it can start from after adolescence. As the hair loss progresses very slowly, patients often does not recognize the hair loss and starts to recognize it when hair loss has progressed considerably.
For medical treatment, finasteride and minoxidil are used in male patients, but finasteride is not effective in female patients, leaving minoxidil as the only option. Finasteride, a competitive antagonist of type 2 5α-reductase, was first developed as a treatment of prostate hypertrophy but was later developed as hair loss drug after finding out that that it can stimulate hair growth. This drug inhibits testosterone from becoming DHT and reduces the level of DHT in the blood and scalp, thereby reducing hair removal.
It has been approved by FDA for 1mg per daily dose in male aged 18 years or older. It was found to improve the number of hair as well as the thickness and growth of hair length within 24 months of treatment (Figure 3). However, such effects faded away within 12 months after discontinuation of the administration. There was no remarkable side effect, except for small number of gynecomastia, even after 5 years of long-term treatment, neither an interaction with other drugs nor special effect on hepatic, renal, bone marrow, and serum lipid levels. Sperm production was not affected and, despite reports of a small number of hyposexuality and erectile insufficiency in the early phase, recent studies found that such side effects were not different from those reported by the placebo group. In principle, Finasteride is not used for women in childbearing age due to the risk of birth defects, but has been shown to be effective in a number of cases of post-menopausal women.
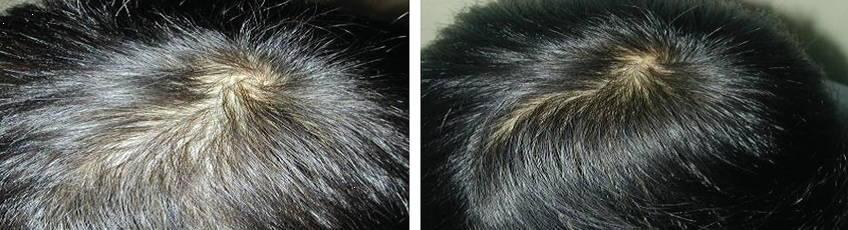
Figure 3. Before and 1 year after administering Finasteride 1mg
Minoxidil is a potent vasodilator, originally developed as an oral antihypertensive drug. After finding out that it caused abnormal hypertrichosis in patients who took this drug for a long period of time, external application experiment was performed to confirm hair growth effect and then it was developed as a hair loss treatment. 1ml of Minoxidil is applied on dried scalp twice a day and left for about an hour until completely absorbed. In general, female patients use 2-3% Minoxidil and male patients use 5% Minoxidil. The hair growth effect is the greatest at 16 weeks after use, along with other effects, such as increased hair volume at the area of hair loss and prolonged growth phase.
Side effects are most common when 5% Minoxidil is used compared to when 2% Minoxidil used. The most commons side effects are scalp irritation, such as dryness, scale formation and pruritus. Hypertrichosis may develop at unwanted areas, especially on the forehead among women or children.
Hair transplantation may be the most complete resolution of hair loss because the transplanted hair can grow permanently; however, the existing hair loss continues, requiring countermeasures. The 25-year-old male patient in (Figure 4) had 3,500 hair transplantation and achieved aesthetic effect after the growth of the transplanted hair.
![]()
Figure 4. Front and center of the head shows growth of 3500 transplanted hairs but the loss of existing hair has progressed on the top of the head.
However, without a post-procedural drug therapy, the existing hair loss progressed abruptly over the next one year, and the patient complained that the therapeutic effect achieved by the hair transplantation was reduced. In this case, the hair transplantation itself was not the issue but patients may express their dissatisfaction when they could not have the expected result. The 23-year-old male patient in (Figure 5) had 4,500 hair transplantation and received finasteride continuously for 2 years after the transplantation. The patient achieved an excellent outcome that would have been impossible only with hair transplantation, and the outcome may be a synergistic effect of transplantation and drug therapy.
![]()
Figure 5. Hair transplantation of 4500 hairs in combination with drug therapy showed synergistic effect.
Taken together, as the existing hair loss tend to continue, the therapeutic effect of hair transplantation declines gradually without combination with a drug therapy. It would be necessary, therefore, to combine hair transplantation with a drug therapy.
- To be continued -
▶ Previous Artlcle : #1. History and Basic Concepts of Hair Transplantation
























