








The following should be confirmed to determine the size and location of donor site before harvesting from the donor site:
1. Donor site density
2. Hair thickness
3. Anagen-telogen ratio
4. Hair color (gray hair) and texture (degree of curliness)
5. Scalp elasticity and thickness
6. Recipient site area and density

[Advertisement] Reandnè Thread Series – Manufacturer: GTG KOREA(www.gtgkorea.com)
Computer-assisted Trichoscan is frequently used to determine donor site density, hair thickness, anagen-telogen ratio, and etc. (Fig. 1).

Figure 1.
In order to determine the size of the donor site to be harvested, the donor site density should be analyzed first, and hair loss area and transplantation density should be determined.
Hair loss area(㎠)×Transplantation density(follucular unit/㎠)=Required number of follucular unit
Donor site density(follucular unit/㎠)×Area to be harvested(㎠)=Number of follucular units to be harvested
Area to be harvested(㎠)=number of follucular units÷donor site density(follucular unit/㎠)
Since the donor site width is determined typically between 1 and 1.5cm, the area to be harvested can be determined by adjusting the length. For example, if the hair loss area is 120㎠ and the recipient site density is determined as 25 follicular unit/㎠, 120㎠×25 FU/㎠=3,000 hairs are required. If the patient’s donor site density is 130 FU/㎠, the donor site area to be harvested is 3000 hairs ÷ 130 hairs/㎠=23.5㎠. If the donor site width is 1.5cm, 23.5㎠÷1.5cm=15.5cm should be harvested.
Let me introduce a simple method to determine recipient site area. First place a wrap on the scalp as shown in the figure below, and mark the hair loss area with a pen. Place the wrap again on a graph paper and count the number of cells (1㎠) to calculate the hair loss area (Fig. 2-1 and 2-2).

Figure 2-1, 2-2.
Scalp elasticity can be divided to hyperelastic, normal or tight scalp. There are various opinions about donor site incision width; I personally try not to exceed 1.5cm, if possible, for normal scalp, or limit the incision width within 1.3 to 1.4cm in young patients in their 20s and 30s so as to minimize scarring. Tight scalp may not be easily sutured even after the incision of only 1cm; hyperelastic scalp may be easily sutured after 2cm or more incision, but it would be reasonable to limit the width to 1.5cm or less to prevent excessive scarring afterward.
When harvesting scalp from the back of the head, it should be hypothesized. The hair loss would progress to Norwood type VII and the scalp may be harvested from the area below that. Since the hair in this area is permanent hair, it will still grow after transplantation. If the scalp was harvested above the area, the scar may be exposed once the male-pattern hair loss has progressed to Norwood type VII, and there is a likelihood of hair loss of the transplanted hair.
The area where the scalp is to be harvested should be sterilized with alcohol and anesthesized. I personally use 1% lidocaine with 1:100,000 epinephrine for donor site anesthesia. Incision is made then with No. 20 surgical scalpel blade until the middle layer of the subcutaneous fat but not into the galeal layer. The blade should be in parallel to the angle of the existing hair so as to minimize the cutting of hair follicle. While lifting one end of the donor site tissue, the donor site is separated from the lower tissue with No. 20 scalpel (Fig. 3).

Fig 3.
Hemostatic measures should be completed before applying suture. If there is an active bleeding from an artery, hemostat clamp is needed. Hemostasis may be maintained after releasing the hemostat before suturing for small blood vessels, but larger blood vessels need ligation with 4-0 vicryl. It is commonly known that cautery should be avoided, if possible.
Methods to reduce donor site scar have changed a lot. After experiencing larger scarring due to hair follicle damage after interrupted subcutaneous suture in the past, I used to do simple interrupted skin suture only, without subcutaneous suture. In case of young patients or patients with hyperelastic scalp with high likelihood of scar extension, I try to reduce the wound tension and thus the width of scar by applying running subcutaneous suture. After various attempts, I prefer the following suturings to reduce donor site scar:
❶ After harvesting the donor site, Trichophytic suture after removing the epidermis and upper dermis 1mm width from the edge of the inferior skin with scissors
❷ Subcutaneous suturing to reduce wound tension and to prevent stretch-back phenomenon
Running subcutaneous suture seems helpful for diminishing the scar by reducing wound tension and stretch-back phenomenon. After inserting a needle of vicryl 4-0 to an end of the incised site, insert the needle horizontal to the deep subcutaneous fat layer below the hair follicle and then horizontal to the other side to make the pattern in the <Fig. 4>, pull the needle out of the skin on the other side and then pull both ends of the thread until the incisions could be brought together so as to reduce wound tension (Fig. 5). After that, simple interrupted suture is performed with 4-0 nylon for skin suturing.
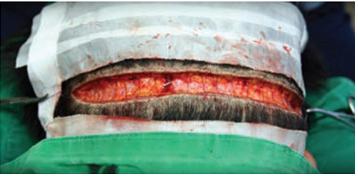
Fig 4.

Fig 5.
Stapler, absorbable mateirla or nonabsorbable material could be used for skin suturing; however, nylon or prolene is often used becauase absorbable material may sometimes induce itching or oozing from tissue reaction.
- To be continued -
▶ Previous Artlcle : #6. Preparation and Local Anesthesia Before Hair Transplantation
























