







The term ‘fractional laser’ comes from the fact that this laser irradiates not all but part of the skin surface. When a company called ‘Reliant’ first developed and commercialized Fraxel, it became a byword for fractional laser. As Botulinum toxin is referred to as just Botox, fractional lasers are commonly termed as Fraxel. Resurfacing lasers, such as CO2 laser and Er:YAG laser, are very effective but requires wound healing period because of deep resurfacing from the skin surface even to part of the dermis. Delayed wound healing or incapability of normal wound healing may lead to serious sequelae, including hypertrophic scar and decoloration. Deeper laser resurfacing means longer duration of erythema and postinflammatory hyperpigmentation (PIH) in Asians, causing much discomfort in social life. Low power infrared lasers were developed to overcome such disadvantages of resurfacing lasers and for skin contraction. Although they might induce fewer side effects such as erythema or hyperpigmentation, they lacked sufficient therapeutic effect, which was a disappointment for both doctors and patients, making it a less attractive option. Fractional laser was developed to achieve both the safety and comfort of infrared lasers and the therapeutic effect of skin resurfacing lasers.
Compared to resurfacing lasers which may cause problem by removing all of the epidermis, fractional laser leaves most of the epidermis intact and delivers heat deep into the dermis to induce skin contraction. The minute laser (micropore; 70150μm in diameter) so small that it irradiates 100 to 400 beams per pass per skin area, which accounts for only 5-10% of total area.

[Advertisement] COPPER BROMID(Yellow/Green Laser) – Manufacturer: BISON(www.bisonmedical.com)
According to the data on original Fraxel by Reliant, the laser beam produces a kill zone, the central pore with an irreversible heat injury (central necrosis), and a coagulation zone, the surrounding area with reversible protein denaturation from less heat. The kill zone at the center and coagulation zone are called Micro Thermal Zone (MTZ), which affects the epidermis and upper dermis (300-750μm in depth) by 100-400 small beams per 1cm2 of Fraxel irradiation. The irradiation covers about 5-10% of skin area per pass and 6-10 repeated passes do not exceed 40-50% of the area, preserving more than half of the skin surface.
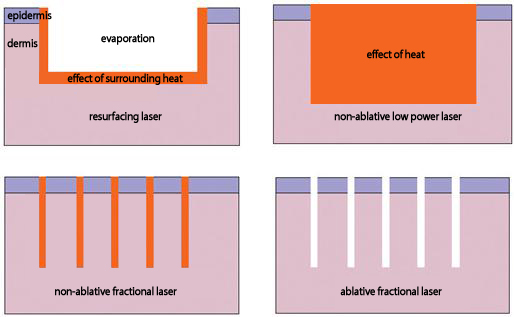
Figure 1. Comparison of the therapeutic mechanism among resurfacing laser, non-ablative low power laser, non-ablative fractional laser and ablative fractional laser (ablative fractional beam has thermal effect to the surrounding area)
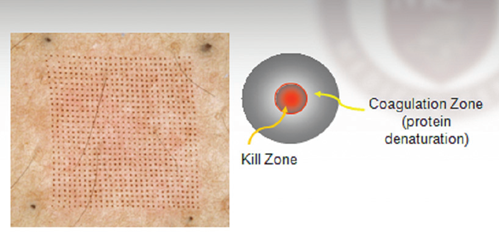
Figure 2. Micro Thermal Zone (MTZ) of Fraxel(provided by Reliant)
Fraxel is a non-ablative fractional laser, delivering heat only without skin resurfacing of the irradiated area. The epidermis regenerates from the surrounding epidermal cells and goes through very rapid recovery by epithelization within 24 hours. The dermis damaged by heat undergoes gradual collagen remodeling and skin contraction. Non-ablative fractional lasers like Fraxel do not induce immediate skin contraction at the time of irradiation but show delayed skin contraction by dermis change.
Fraxel is a 1,550nm infrared Er:Glass laser, with moisture affinity and nonselective absorption in tissue. It used blue dye coating to maximize laser absorption, but recent fractional lasers uses gels only, without any special dye coating. There are a number of non-ablative fractional lasers, but a good fractional laser does not leave a clear stain or spreading to the sides when tested on a black paper or wooden tongue depressor.
Non-ablative fractional laser leaves erythema and edema which last for about 1 day. Patients can live their normal daily lives, including washing and putting on a make-up, from the next day, without any down time in social life. Patients rarely complain about postinflammatory hyperpigmentation (PIH) unless they have melisma or sensitive skin.
Despite lack of effect on epidermal lesions, non-ablative fractional lasers are effective for gradually lightening pigmented lesions and somewhat improves hypertropic, atrophic and hypopigmented scars. The skin contraction effect also improves wrinkles and acne scars but requires more than 3-5 courses of repetitive treatments every 3-4 weeks because the effect is weak. Non-ablative fractional lasers are safe without skin resurfacing, more effective than low output infrared lasers but not as dramatically effective as resurfacing lasers, which is why ablative fractional laser was developed by integrating ablative CO2 laser and Er:YAG laser with fractional effect.
Ablative fractional lasers have characteristics of both fractional laser and resurfacing laser. CO2 (10,600nm) fractional laser induces partial minute skin resurfacing by vaporizing both tissue and water. Upon the irradiation of a small beam from Fraxel, both the epidermis and dermis vaporize in the form of Micro-Ablative Column (MAC) and the surrounding area contracts by thermal effect.
The vaporized MAC undergoes wound healing in 2 days, regeneration of the epidermis (epithelization) within 2 days, and the dermis area affected by thermal effect is also replaced by collagen remodeling. Erythema and edema settle down within 2-3 days, enabling washing and putting on a make-up in 2-3 days. Discomfort and daily life can be minimized by weekend procedure. Ablative fractional laser shows immediate notable skin contraction effective compared to non-ablative fractional laser.
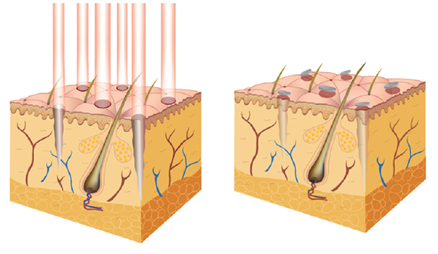
Figure 3. Ablative fractional laser (eCO2): the process of micro ablative column (MAC) on the left, epithelization on the left, and collagen remodeling of the dermis, provided by LUTRONIC
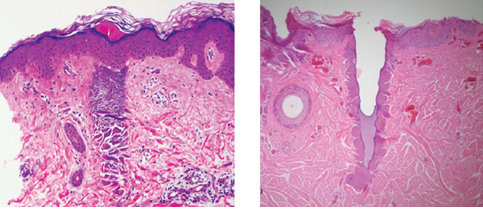
Figure 4. Cross-sectional histological findings of non-ablative fractional laser (Left) and ablative fractional laser (Right), provided by LUTRONIC
Ablative fractional lasers irradiate 100 to 200 small beams per 1cm2 and single pass is enough, not requiring repetitive irradiations. When the second course of treatment is needed, the interval should be longer than non-ablative fractional laser, typically 2 months for the face and 3 months for the extremities and the trunk. The parameters of fractional laser are determined by adding pulse per unit area with energy per pulse. For non-ablative fractional laser, 200-400/cm2 pulse, 30-50mJ/pulse, 3-4 passes, and overall 5,000-20,000mJ/cm2 are used. For ablative fractional laser, 80-150/cm2, 50-60mJ/pulse, 1 pass, and overall 5,000~20,000mJ/cm2 are used. Overall high energy can be commonly applied to the face but the overall energy should be lowered for the trunk and extremities.
Non-ablative fractional laser is safe and hardly affects daily life, while ablative fractional laser has superior effect in improving wrinkle and scar. Dermatologists generally prefer non-ablative fractional laser, compared to plastic surgeons who tend to prefer ablative fractional laser.
I once had an opportunity to test Fraxel by Reliant and eCO2 laser by Lutronic upon their requests for advice. According to animal tests, epithelization was quicker with non-ablative fractional laser and skin contraction effect with ablative fractional laser; both lasers increased epidermal and dermal thicknesses, dermal collagen remodeling and density of collagen fibers.
Clinical trials were mostly conducted in patients with wrinkle and acne scar. Acne scar was treated by 4-5 courses of non-ablative fractional laser treatment and 2-3 courses of ablative fractional laser treatment; despite fewer numbers of treatments, ablative fractional laser showed superior therapeutic effect than non-ablative fractional laser.
An efficient ablative fractional laser should be able to generate MAC with similar diameters between the skin input area and the bottom penetrated area; inefficient ablative fractional laser generates MAC with wide input and narrow penetration.

Figure 5. Traumatic scar improved by early fractional laser (1 course of non-ablative fractional laser treatment and 2 courses of ablative fractional laser treatment from 1 month after suffering the injury)
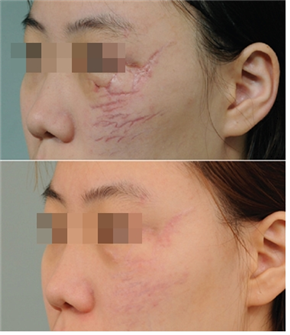
Figure 6. Scar from cleft lip reconstruction improved by ablative fractional laser
According to eCO2 laser by Lutronic, ablative fractional laser can reach to the lower dermis (2.4mm) when the output is high. Therefore, the therapeutic effect can be enhanced by combining ablative fractional laser with other lasers. For example, the duration of treatment can be shorted by combining ablative fractional laser with Q-switch laser when treating the nevus of Ota, a deep dermal pigmented lesion. The therapeutic effect for superficial capillary malformation (port wine stain) can be enhanced by combining ablative fractional laser with vascular laser.
One advantage of fractional laser than resurfacing laser is that it can improve burn scar, striaedistance and hypopigmented scar, which was impossible with resurfacing laser. Side effects, such as hypertrophic scar formation or decoloration, were often associated with resurfacing laser, but fractional laser shows superior effect for such scar as well. Fractional laser also enhances skin contraction and elasticity, flattens scar, and neutralizes the color of scar. Table 2 compares the characteristics among resurfacing laser, non-ablative fractional laser and ablative fractional laser. The shape of lesion and patient’s needs should be considered when selecting a laser device for a more superior and satisfactory therapeutic outcome. We will discuss about lasers for vascular lesions in the next chapter.
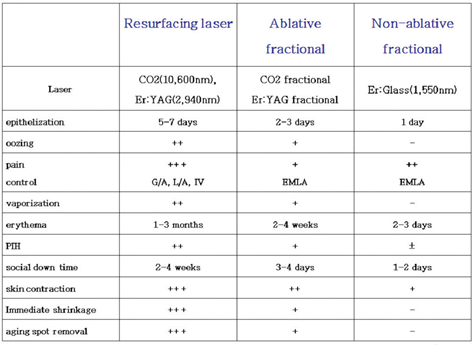
Table 2. Comparison of characteristics among resurfacing laser, ablative fractional laser and non-ablative fractional laser
- To be continued -
▶ Previous Artlcle : #4. Scar Type and Laser Therapy
▶ Next Artlcle : #5. Fractional Laser
























